Pediatric Cardiology Part 2
A Chapter in Core Concepts of Pediatrics, 2nd Edition
shraf Aly MD, PhD
This chapter is designed to cover the essential highlights of pediatric cardiology electrocardiogram (EKG). It is the second part of the Cardiology Chapter in Core Concepts of Pediatrics. It is important that every pediatric provider, not just the cardiologist, understands the basic hemodynamics of the heart and the integration of the cardiovascular system with other body systems.
|
The authors acknowledge the contribution of Dr. Vidit Bhargava for assistance with image creation. |
S. Bhatia, MD, L. Yun, S. Munir, M.E. Gomez, MD A. Aly, MD, PhD
Before you read the EKG, look for:
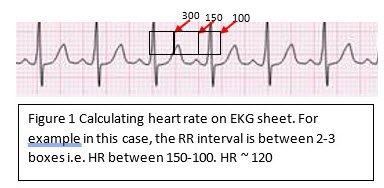
1. Heart rate: The standard paper speed is 25 mm (5 large squares)/sec. This means that if the interval between two beats (R-R) is 5 large squares, the HR is 60 beat/min.
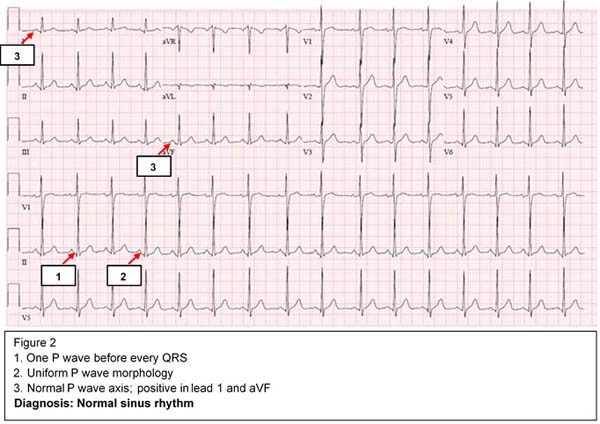
2. Rhythm: The cardiac myocytes have an inherent automaticity and can generate an electric impulse. The SA nodal cells have the fastest automaticity (pacemaker) and hence control the heart rate and rhythm. There are 4 levels of conductions and potential pacemakers in the heart from fastest to slowest: SA node → atria → AV node → ventricles. If the rhythm is not sinus, we have to determine the origin of the pacemaker and where the impulse is initiated.
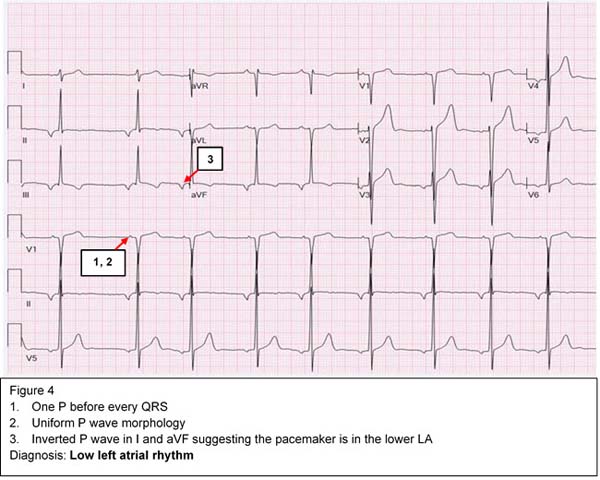
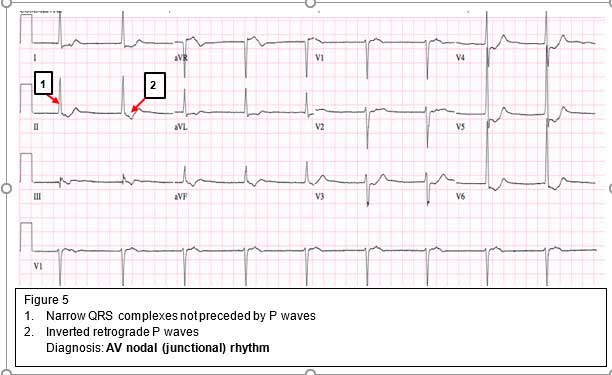
If the sinus node fails to initiate the impulse, an atrial focus will take over as the pacemaker, which is usually slower than the NSR. When the atrial focus fails, the AV node will take over. Subsequently, if the AV node fails, the ventricular focus, which is the slowest, will take over as a pacemaker. Each time the focus is downgraded, the heart rate becomes slower based on the inherent automaticity of the pacemaker.
3. Axis: Determine both P wave and QRS axes. The net summation of positive and negative deflection is used to determine the axis. Look for two perpendicular leads (usually lead I and aVF) to determine in which quadrant the axis is located.
a) If QRS is positive in lead I and positive in aVF, the axis is in the left lower quadrant (0-90 degrees), which is normal
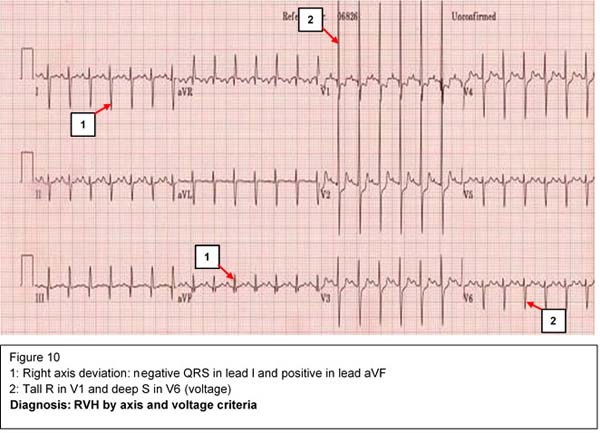
b) If QRS is negative in lead I and positive in aVF, the axis is in the right lower quadrant (90-180 degrees). This represents right axis deviation which can be normal in children.
c) If QRS is positive in lead I and negative in lead aVF, the axis is in the left upper quadrant (-90- 0). This represents left axis deviation.
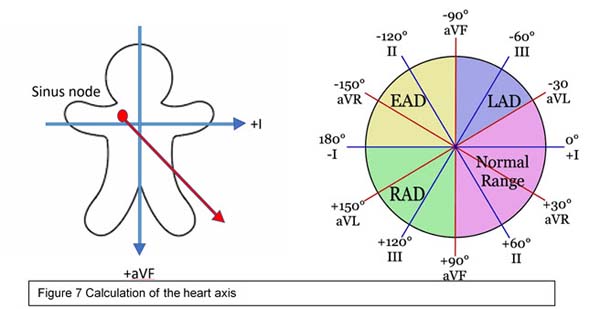
d. If QRS is negative in lead I and negative in lead aVF, the axis is called indeterminate. Precordial leads may determine if it is an extreme right or left axis deviation.
4. Durations/Intervals:
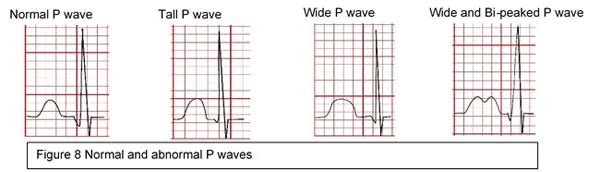
a) P wave: Represents atrial depolarization. Normally it is 2.5 mm wide and 2.5 mm high.
b) PR interval represents a delay in conduction in the AV node. It varies with age and heart rate and is usually <0.2 sec at any age.
c) QRS duration: Represents ventricular depolarization. Normally 2 small squares or 0.08 sec.
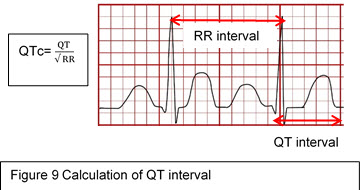
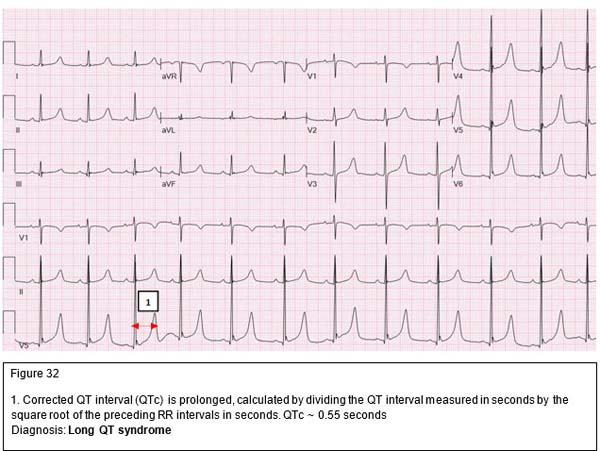
d) QT interval (measured from the beginning of Q to the end of T wave) represents both ventricular depolarization and repolarization
• QTc is the QT interval corrected for the heart rate. QTc=QT (in seconds)/square root of preceding RR interval (in seconds).
• See causes of long QT syndrome below.
5. Chamber Hypertrophy/Enlargement
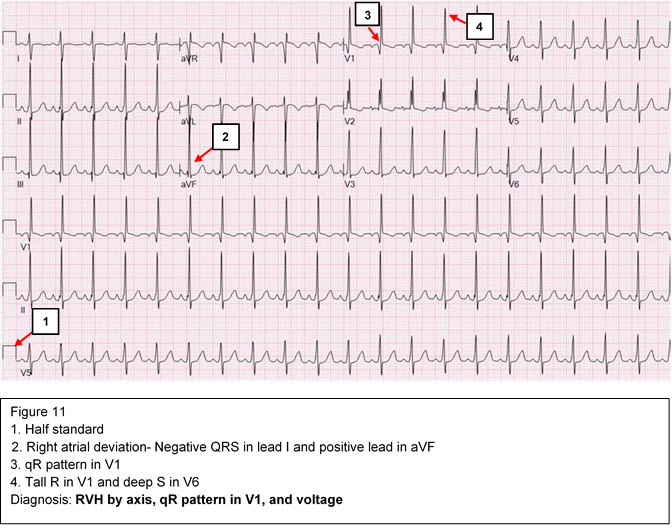
a) Right ventricular hypertrophy (RVH):
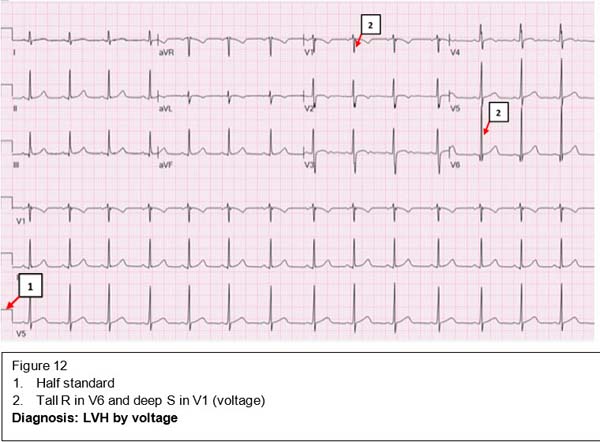
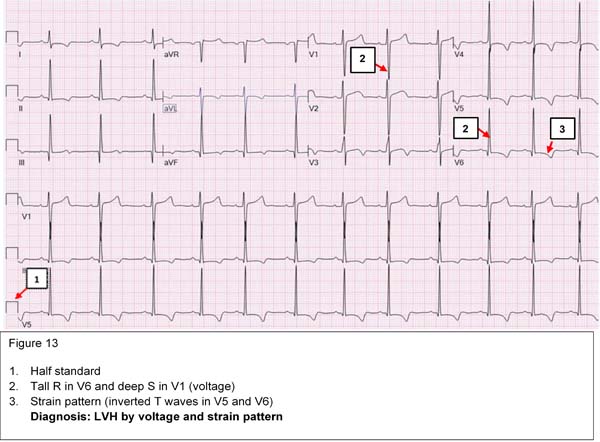
b) Left ventricular hypertrophy (LVH): Criteria are not as well defined as RVH
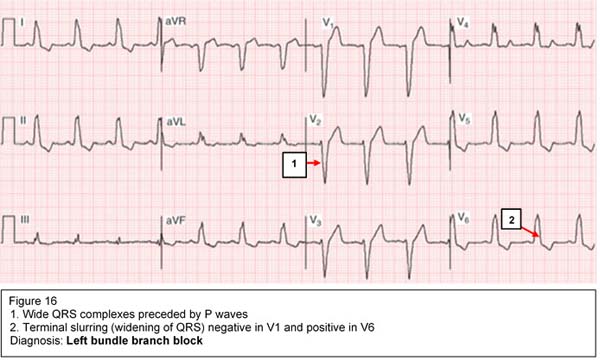
6. Bundle Branch Block (delay in conduction in either the right or left bundle of His)
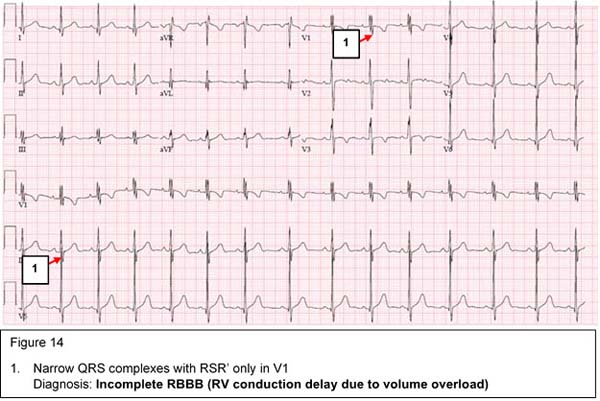
Incomplete right bundle branch block (iRBBB, RV conduction delay/ RV volume overload)
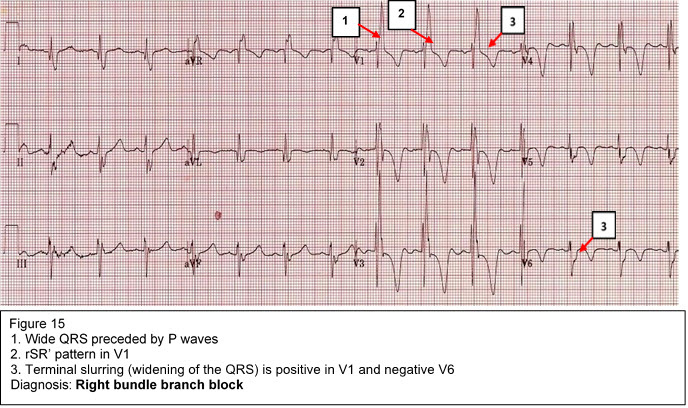
Complete right bundle branch block
Complete left bundle branch block
Arrhythmias are defined as disturbances in heart rate and/or conduction. Arrhythmias result from abnormal impulse formation, abnormal impulse conduction, or both. Arrhythmias may occur in children with normal hearts and/or may be associated with CHD, medications or electrolyte disturbances.
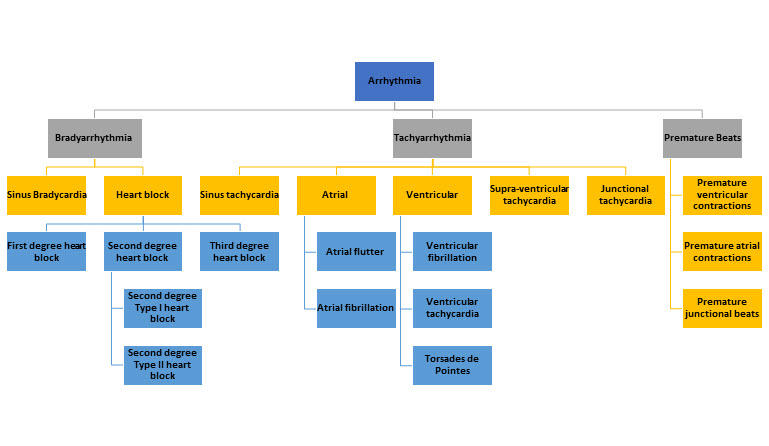
Types of Arrrhyhimias
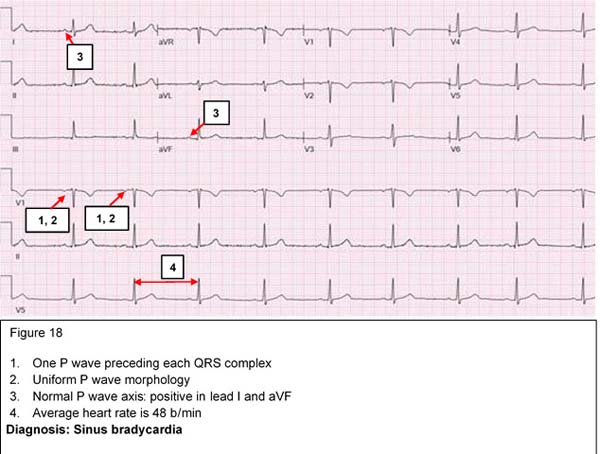
The normal range of heart rate depends on the age of the individual, ranging from 120-160 beat/min in the newborn to 60-80 beat/min in the adult. Trained athletes may normally have sinus bradycardia due to increased vagal tone. Pathological sinus bradycardia is usually secondary to an underlying condition such as hypothyroidism or medications such as beta-blockers.
Asymptomatic physiologic sinus bradycardia requires no treatment. In symptomatic bradycardia, the underlying cause should be treated and a pacemaker placement may be considered if there is no response to medical therapy.
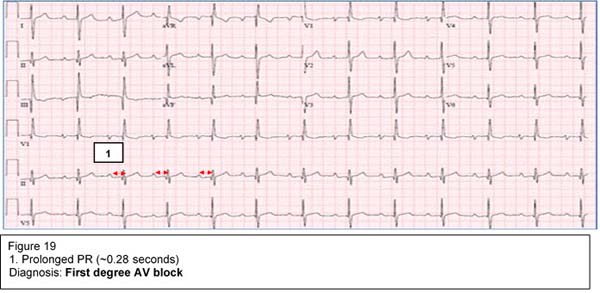
First degree AV block
This indicates prolongation of the PR interval more than 95th percentile for age and heart rate. At any age, PR interval > 0.2 seconds is considered prolonged.
Causes include:
It is usually reversible and does not require any treatment. First degree AV block could be one of the cardiac manifestations of rheumatic fever.
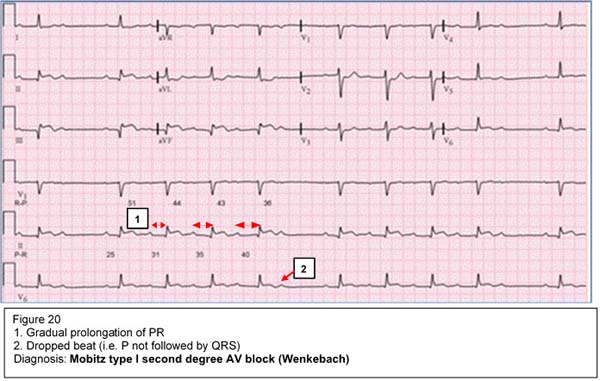
Second degree AV block
This is secondary to an intermittent failure of conduction through the AV node so that some P waves are not followed by QRS complexes.
Mobitz type I (Wenckebach) is a gradual prolongation of the PR interval until there is a P wave that is not conducted (not followed by a QRS complex). It is usually benign and may be seen in the presence of increased vagal tone, during sleep or in trained athletes.
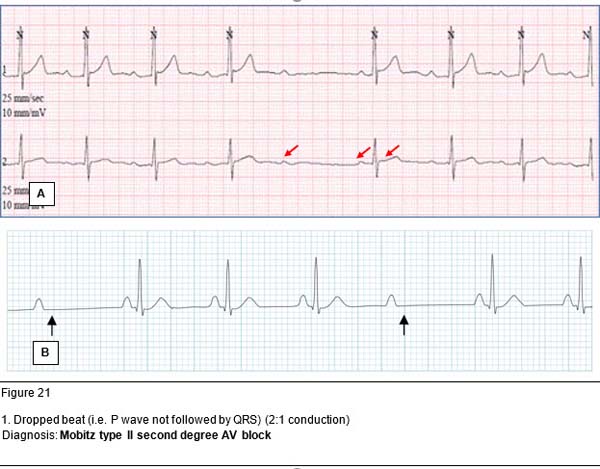
Mobitz type II is sudden loss of AV conduction (two or more P waves before QRS complexes). It is more serious as it may progress to a complete AV block. Implantation of a pacemaker may be considered in symptomatic patients.
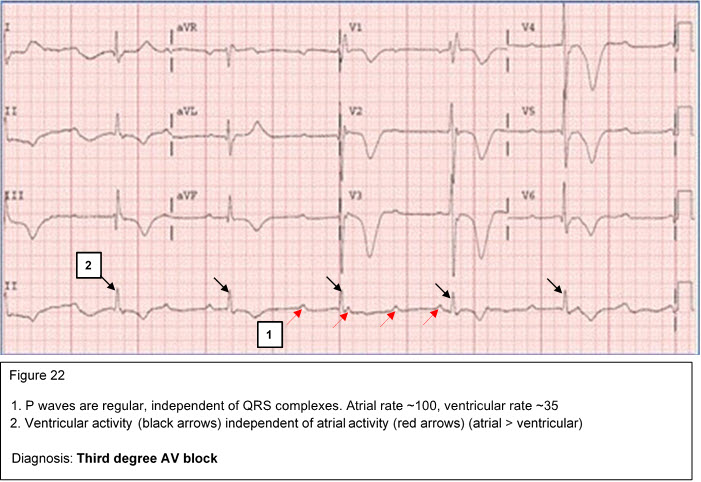
Third degree (complete) AV block (atrioventricular dissociation)
Complete AV block represents complete atrioventricular dissociation with no correlation between the atrial and ventricular electrical activity. The ventricular rate is significantly slower than the atrial rate. A pacemaker placement is warranted in symptomatic patients. This condition may be seen in infants born to mothers with systemic lupus erythematosus (SLE).
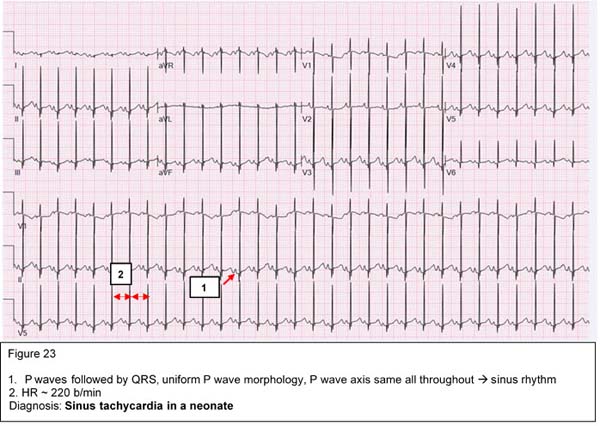
Sinus tachycardia is characterized by narrow fast QRS complexes that are preceded by normal P waves. Sinus tachycardia may be a physiologic response to exercise, anxiety, fever, hypovolemia, hypoxemia or hyperthyroidism. A good rule of thumb to remember for fever is 1 degree Celsius increase in temperature accounts for ~10 b/min increase in HR. Maximum physiologic HR is 220 bpm age in years.
|
Maximum heart rate =220 - age in years |
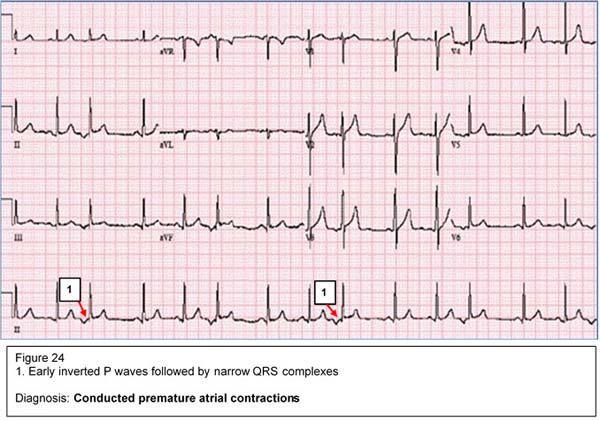
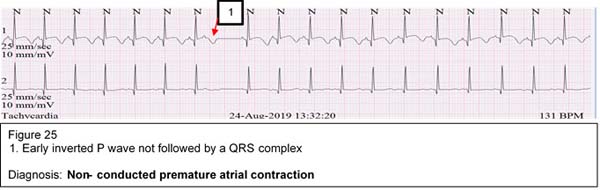
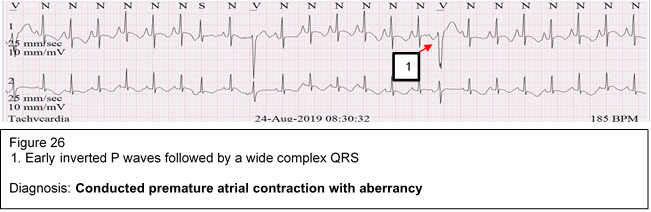
PAC's represent an early atrial electrical activity outside the SA node. PAC's may appear in one of three forms:
PAC's are commonly seen in infants and usually disappear with increasing age. It is usually benign and needs no treatment.
SVT is characterized by a narrow QRS complex tachycardia with a heart rate of 250-350 beat/min. It is commonly seen in children with normal hearts but may be associated with some CHD such as Ebstein anomaly. SVT may be caused by an accessory pathway between the atria and the ventricles or by a reentry circuit within the AV node. In infants, SVT presents with poor feeding, irritability, sweating and respiratory distress. Prolonged SVT may lead to CHF due to coronary insufficiency.
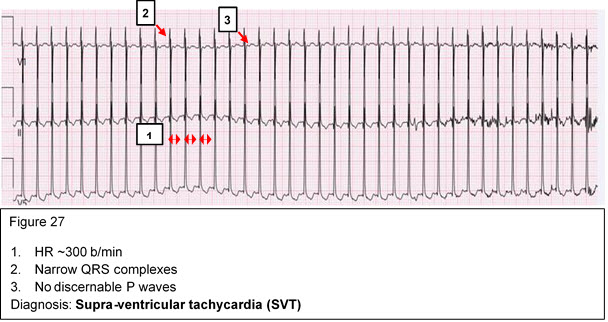
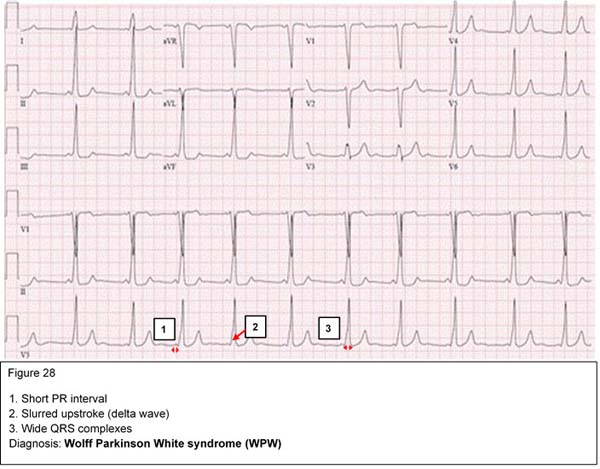
Compensated SVT should be treated promptly with vagal maneuvers such as application of ice to the face. If this is unsuccessful, then adenosine should be administered intravenously. Children with uncompensated SVT should undergo cardioversion. Wolff Parkinson White (WPW) syndrome is an example of pre-excitation due to an accessory pathway between the atria and ventricles. It is characterized by short PR intervals, delta waves, and wide QRS complexes.
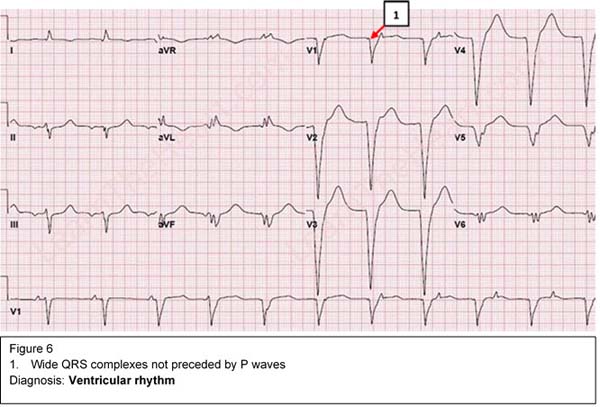
Ventricular arrhythmias are characterized by wide QRS complexes that are not preceded by P waves, and abnormal T waves. The symptoms depend on the heart rate and are usually due to poor ventricular filling. This is a potentially serious dysrhythmia and synchronized cardioversion is commonly indicated.
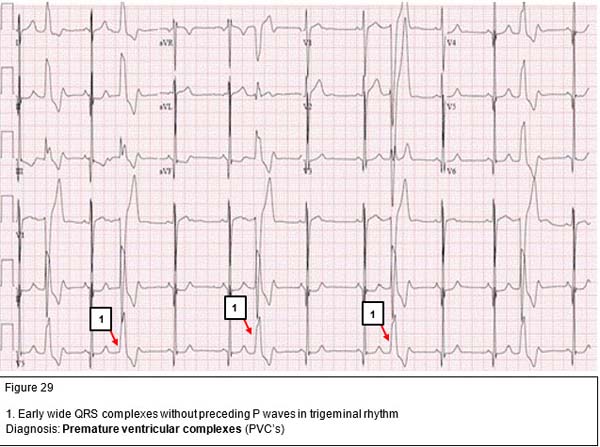
PVC's are early, wide QRS complexes that are not preceded by P waves. Isolated unifocal PVC's originate from the same spot in the ventricles and have a uniform morphology. They are usually benign in nature and disappear as the heart rate increase with exercise. On the other hand, multifocal PVC's have different morphology as they originate from different foci in the ventricles. They usually occur in diseased myocardium and their frequency often increases with exercise.
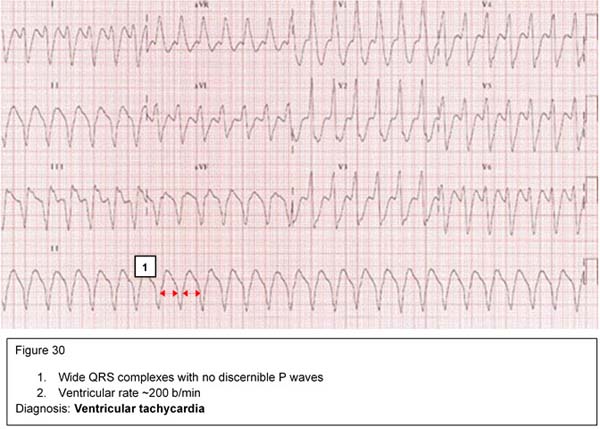
VT is a rapid, wide QRS-complex tachycardia with a heart rate 150-250 beat/min. It is a serious condition that may result from drug toxicity (digoxin), myocarditis or severe metabolic derangement. It should be treated promptly with synchronized DC cardioversion if the patient is hemodynamically unstable. Stable VT may be treated with IV lidocaine infusion. Oral amiodarone may be used for outpatient management.
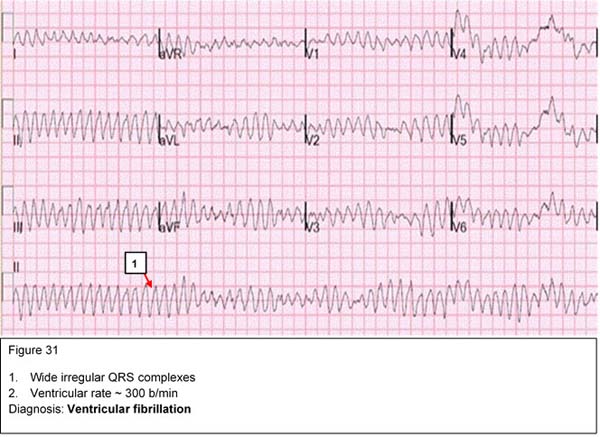
VF is a serious and terminal cardiac rhythm characterized by irregular, wide bizarre shaped QRS complexes. It needs urgent treatment with unsynchronized DC cardioversion.
The QT interval represents both ventricular depolarization and repolarization. The QT interval varies with heart rate. The faster the heart rate, the shorter the QT interval. The corrected QT (QTc) interval is calculated by dividing the measured QT in seconds by the square root of the preceding R-R interval in seconds. A corrected QT greater than 0.46 seconds is considered prolonged. In normal neonates, the QTc may be 0.50 seconds in the first few days of life.
LQTS is an inherited condition characterized by syncope, seizures, palpitations or even sudden death. There are four different classes of patients with LQTS:
|
Antipsychotics |
Antiarrhythmics |
Tricyclics |
Other antidepressants |
Antihistamines |
Others |
|---|---|---|---|---|---|
|
Chlorpromazine |
Quinidine |
Amitriptyline |
Citalopram |
Diphenhydramine |
Erythromycin |
|
Haloperidol |
Procainamide |
Doxepin |
Escitalopram |
Loratadine |
Clarithromycin |
|
Droperidol |
Disopyramide |
Imipramine |
Venlafaxine |
Terfenadine |
Quinine |
|
Quetiapine |
Flecainide |
Desipramine |
Bupropion |
|
Chloroquine |
|
Olanzapine |
Sotalol |
|
|
|
Hydroxychloroquine |
|
Thioridazine |
Amiodarone |
|
|
|
|
Table 2: Common drugs which may cause QT prolongation
Pathophysiology
Congenital long QT syndrome may be caused by an imbalance of the sympathetic innervation in the heart especially the stellate ganglion or derangements in the cardiac ion flow, resulting in prolongation of the action potential. During the latter phase of the action potential, the myocardium is very excitable and may develop arrhythmia if stimulated electrically or mechanically. If a PVC occurs during this phase of the action potential (R on T phenomenon), a delayed after-depolarization develops in the form of a specific polymorphic ventricular arrhythmia (Torsades de pointes).
No discernable P waves, wide QRS complexes twisting around isoelectric axis
Dianosis: Torsades de pointes
Clinical
Most patients are asymptomatic. Symptomatic patients present with episodic dizziness, palpitations, syncope, seizures, and/or cardiac arrest. Patients with long QT syndrome can develop Torsades de pointes, bradyarrhythmias, or AV block. This can be triggered by exercise, emotions or loud noises.
Making the Diagnosis
Management
LQTS is a serious condition. The risk factors for sudden death include long QT > 0.55 seconds, family history of sudden death, bradycardia for age, and a prior history of symptoms. Any medications that may cause QT prolongation should be discontinued.
Treatment is aimed at preventing conversion to other possibly fatal arrhythmias. Beta-blockers are the mainstays of medical management. An implanted cardioverter-defibrillator (ICD) is often used as a nonpharmacological treatment. Other treatment modalities include permanent dual chamber pacemaker and left cardiac sympathetic denervation.
Click here to download or open PowerPoint Show link
2007 Guidelines From the American Heart Association.
Abbreviations for CardiologyChapter
American Academy of Pediatrics
Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease:
Scientific statement from American Heart Association
Evaluation of the Cyanotic Newborn: Part1 - A Neonatologist's Perspective UTMB password required
Evaluation of the Cyanotic Newborn: Part2 - A Cardiologist's Perspective UTMB password required