Newborns and their families are cared for by either general pediatricians or neonatology specialists. This chapter is designed for the student to learn the basics of newborn care from the perspective of the general pediatrician.
Newborns and their families are cared for by either general pediatricians or neonatology specialists. This chapter is designed for the student to learn the basics of newborn care from the perspective of the general pediatrician.Neonatology
A Chapter in Core Concepts of Pediatrics, 2nd Edition
Manuela J. Murray MD and Joan Richardson MD
Newborns and their families are cared for by either general pediatricians or neonatology specialists. This chapter is designed for the student to learn the basics of newborn care from the perspective of the general pediatrician.
Birth is the most dangerous physiological event in an individual's life. Although most newborn babies are normal, the physician needs to be aware of the special vulnerabilities of the newborn and the physiologic changes that take place as the neonate makes the dramatic transition from a protected uterine environment to independent life.
After completing this chapter, the student should be able to:
Ideally, all parents should have a meeting with the prospective pediatrician some time prior to the anticipated date of delivery. From the pediatrician's perspective, care of the newborn baby begins with this prenatal interview. The primary goals of this meeting are for both parties to establish a level of comfort with each other and to earn their expectations of each other. For example, most pediatricians do not attend uncomplicated deliveries, so the parents need to be told that the pediatrician will most likely see them the next morning. In addition, the pediatrician needs to evaluate the attitude of the parents towards the pregnancy and to have them review some of the decisions that they will have to make before and immediately following the birth of the baby. This is also an opportunity for the pediatrician to inquire about events in the prenatal history that might have an impact the health of the baby.
Elements of the prenatal interview include:
|
More information on Prenatal Interview |
|
Breast or Bottle? From Kidshealth Circumcision: AAP Policy
|
Prior to examining the newborn baby, it is important to review the records of the baby and the mother for information that might predict pathology in the newborn. Information on the history of the pregnancy, labor, and the delivery has implications for the health of the newborn.
|
More Info: Low APGAR score |
||||||||||||||||||||||||
|
A low Apgar score may be due to intrauterine asphyxia, hypovolemia, drugs administered to the mother that depress fetal respiratory efforts, severe perinatal infection, or congenital abnormalities involving the lungs, heart, of the central nervous system.
The one minute Apgar score serves as a guideline for the degree of intervention. The five-minute score is an indicator of the efficacy of the resuscitative efforts, if any were necessary. In and of itself, the one- and five-minute Apgar scores are not good predictors of long-term outcome, but may predict a complicated neonatal course, which then increases risk for poor long-term outcome. |
Make your own mnemonic for remembering this list. The list has:
1 A: Apgar
1 B: Birthweight
2 D's: Diabetes, Drugs (legal, illegal, alcohol, smoking)
2 C's: Cord (prolapse, around the neck), Caesarean
3 F's: Fluid x2 (too much, too little) fetal distress
1 H: Hypertension, (toxemia, renal disease)
1 I: Infection (intrauterine or acquired from birth canal)
2 M's: Multiple pregnancy, Meconium
1 P: Prenatal care
1 R: Rupture
1 T: Term
|
Need a break? Read about mnemonics and Greek mythology |
|
More Information on Fetal Circulation |
|
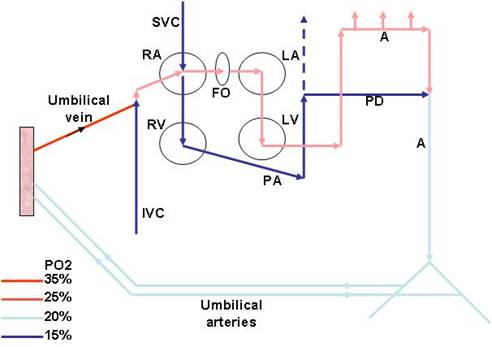
Diagram by A. Kalia In the fetus, oxygenated blood from the placenta enters the umbilical vein and flows into the inferior vena cava (IVC) where it mixes with blood returning from the lower body. From the IVC, blood enters the right atrium and preferentially flows across the open foramen ovale to the left atrium; this blood is then ejected by the left ventricle into the aorta and supplies the coronary arteries and the upper body, including the carotids. Blood that is returned from the upper body by the superior vena cava is preferentially directed to the right ventricle and ejected into the pulmonary artery. The pulmonary vascular resistance in the fetus is high, and the most of this blood blood is shunted across the ductus arteriosus into the aorta and travels to the splanchnic area and the lower body. Much of this blood is routed via the umbilical arteries to the placenta for reoxygenation. Onset of respiration: Prior to birth, the lungs are filled with fluid and receive only 10 to 15% of the total cardiac output. With the onset of respiration, there is expansion of the lungs with air, a sharp decline in pulmonary vascular resistance, and an increase in pulmonary blood flow. Within the first minutes of life, much of the fluid in the lungs is removed by the lymphatics and by the thoracic squeeze resulting from vaginal delivery. Increase in the pO2, a decline in the pCO2, increased in pH and release of bradykinin and prostaglandins also contribute pulmonary arterial dilatation at birth. Pulmonary blood flow increases 8-10 fold, as does the volume of blood returning to the left heart, resulting in increased ventricular output. Cardiovascular changes: Before birth, distribution of left atrial blood between the tricuspid valve and the foramen ovale means that the two ventricles act in parallel. For the heart to function as two pumps in series - the pulmonary circulation and the systemic circulation - direct communications between the right and left sides of the circulation must be closed. After the blood flow from the placenta is removed from the circulation, blood flow to the right atrium decreases. At the same time, blood flow to the left atrium increases because of increased venous return from the pulmonary circulation. The increase in left atrial pressure relative to right atrial pressure closes the valve-like flap overlying the foramen ovale in the left atrium. The ductus arteriosus contains smooth muscle that is maintained in a relaxed state by the action of prostaglandin E1. After birth, serum levels of prostaglandin E1 fall and in most term infants, functional closure of the ductus occurs within the first 12 hours of life. If the ductus remains open, the flow through it will be reversed because of the increase in left ventricular output and aortic pressure. A patent ductus arteriosus leads to excessive pulmonary blood flow and may result in right heart failure. In this situation, indomethacin, an anti-prostaglanding agent, is used to try to achieve closure of the ductus. On the other hand, certain congenital cardiac malformations, such as pulmonary atresia, require patency of the ductus arteriosus to maintain pulmonary blood flow. In this situation, prostaglandins may be infused intravenously to keep the ductus open until surgery can be performed. |
In summary, prior to birth, the placenta is the conduit that provides oxygen and nutrition to the fetus. In the fetal circulation, pulmonary vascular resistance is high and right ventricular output is shunted across the ductus arteriosus into the systemic circulation, bypassing the lungs. At birth, dramatic changes occur in the fetal circulation that allow transition to a lung-based gas exchange.
Pulmonary vascular resistance falls and the ductus arteriosus closes. Right ventricular output now circulates through the lungs before entering the systemic circulation via the left atrium.
Changes also occur in other organ systems. Availability of oxygen from the lungs is better than from the placenta. Enzyme systems are activated in the liver. For example, glucoronyl transferase activation is essential for conjugating the bilirubin produced from the disintegrating RBCs. The kidneys assume responsibility for fluid and electrolyte homeostasis. The immune system has to mature.
![]()
Term
Gestational age
Gestational age can be calculated by the date of the last menstrual period and also by examination of the newborn infant using the Dubowitz or Ballard score. The Ballard score is an abbreviated version of the Dubowitz score, especially useful for estimation of gestational age in premature babies.
|
More Info: Ballard Score from Medcalc |
|
Ballard Score from Medcalc
|
A pediatrician is usually not present at a normal delivery.
|
More Info: APGAR Score |
||||||||||||||||||||||||
|
The Apgar scoring system was developed in 1951 by Dr. Virginia Apgar to evaluate the baby's cardiovascular system immediately after birth and to identify babies at risk for future complications. The Apgar score is determined by evaluating the newborn baby on five criteria, each assessed on a scale from zero to two, then summing up the five values. The resulting Apgar score can range from zero to 10. The baby is scored twice - at one minute and again at five minutes. Most babies will have a one-minute score of 8 of 9. A low Apgar score may be due to intrauterine asphyxia, hypovolemia, drugs administered to the mother that depress fetal respiratory efforts, severe perinatal infection, or congenital abnormalities involving the lungs, heart, of the central nervous system.
The one-minute Apgar score serves as a guideline for the degree of intervention. The five-minute score is an indicator of the efficacy of the resuscitative efforts, if any were necessary. In and of itself, the one- and five-minute Apgar scores are not good predictors of long-term outcome, but may predict a complicated neonatal course, which then increases risk for poor long-term outcome.
Apgar from National Library of Medicine Apgar from MedCalc
|
Immediately after delivery, the infant is wrapped in a sterile towel, wiped dry, placed in a slightly head-down position under a radiant warmer and given oxygen if necessary.
The airway is cleared by aspirating the nose and throat gently with a rubber bulb or suction catheter and the infant is stimulated if respirations are not vigorous. The heart sounds and lungs are auscultated and excursion of the chest is observed. The Apgar score, which reflects newborn health, is determined at one and five minutes. The baby is given to the mother for skin to skin contact for the first hour (kangaroo care) and remains with the mother for the duration of the hospital stay (rooming in).
If complications are anticipated (multiple pregnancy, meconium stained amniotic fluid, evidence of fetal distress, prematurity), the pediatrician is usually called to be present in the delivery room.
The first four of the following steps apply to the delivery room care of all babies. Steps five through ten may be needed if the infant is depressed or asphyxiated.
Management in the post-resuscitation period should include close monitoring of vital signs, blood glucose level, and arterial blood gases. Some infants will require mechanical ventilation. Feedings often need to be delayed and fluids provided intravenously. Infants with seizures will require anticonvulsant therapy.
|
More Information on hemorrhagic disease |
|
Hemorrhagic disease from Lucile Packard Children's Hospital
|
![]()
 The purpose of the newborn physical examination is to assess the baby's transition from intrauterine line to extrauterine existence and to detect congenital malformations and actual or potential disease.
The purpose of the newborn physical examination is to assess the baby's transition from intrauterine line to extrauterine existence and to detect congenital malformations and actual or potential disease.
The baby should be examined briefly immediately after birth. This should be confined to quick assessment of respiration, circulation, temperature, neurological status, and screening for anomalies or disease that might mandate emergency treatment. The initial examination should be done with minimal disturbance to the baby, taking particular care to prevent excessive cooling from exposure.
A complete examination should be performed within the first 24 hours and again at discharge from the nursery. The full examination should be performed when the baby is quiet. The baby should be observed from a distance before being touched since a great deal can be learned by observing the infant's spontaneous activity. See, then touch.
Auscultate the heart and chest and feel the pulses before the baby begins to cry, and then proceed systematically to the rest of the examination.
Posture: The normal healthy newborn demonstrates flexion of the legs and arms when supine. Lack of this posture might indicate hypotonic conditions such as Down Syndrome or neurologic or muscle disease.
Cyanosis: Mild cyanosis is normal at birth but after the first few minutes of life, the child's tongue and mucous membranes should be pink. Peripheral cyanosis (acrocyanosis) might persist for one to two days. Persistent central cyanosis suggests an obstructed airway, respiratory disease, cardiac anomalies, neurologic depression, and rarely methemoglobinemia.
Jaundice: Jaundice is common after the second day of life. The presence of jaundice within the first 24 hours of life suggests a hemolytic process, and is always abnormal.
Vernix caseosa, a cheesy white covering over much of the body, is normally present at birth.
Lanugo (fine hair) is present on the shoulders and back.
Milia (pinpoint white papules caused by blocked sebaceous glands) are often seen on the nose and cheeks.

Milia
Petechiae on the scalp and face are often seen after a vertex delivery.
Congenital dermal melanocytoses, large gray-blue patches of pigment over the lumbar area, buttocks, or extremities (also known as Mongolian spots) are a common phenomenon in dark-skinned races. These tend to fade over time.
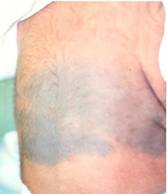
Mongolian Spots
Capillary hemangiomas, common on the upper eyelids, forehead, and the nape of the neck are known as stork bite nevi and also tend to fade with time.

Erythema Toxicum
Erythema toxicum consists of small, yellow papules on a red base and may appear between the second and fourth days of life. These papules contain eosinophils and are seen mostly on the trunk.
Molding of the head by pressure of the maternal pelvis is common after vaginal delivery. Caput succedaneum, a round boggy swelling of the soft tissues of the scalp from accumulation of fluid within the area of pressure from the pelvis during delivery is common. This should be distinguished from a cephalohematoma, which is a sub-periosteal hemorrhage. The former will cross suture lines; the latter does not.
The anterior and posterior fontanelle should be soft to palpation. The anterior fontanelle should be between 1 and 3 cm in size and the posterior fontanelle should admit a fingertip. Following a vaginal delivery, over-riding of the skull bones may temporarily reduce the size of the anterior fontanelle.
The head circumference should be between 33 and 35cm for a full-term infant.
The slant and size of the eyes should be examined. Eyes that slant upward might be a sign of Down Syndrome.
|
Down Syndrome Photo Credit: by AHMA4T Angela Hampton Picture Library / Alamy Stock Photo
|
|
Large eyes suggest congenital glaucoma, a condition that requires early treatment to preserve vision. Eyes that are too close together are suggestive of fetal alcohol syndrome.
Hemorrhage in the subconjunctival and retinal area is common with vertex delivery and has no significance. The pupillary light reflex and a red reflex of light from the retina should be checked with a flashlight or ophthalmoscope. Pupillary opacity indicates congenital cataracts and a white reflex suggests retinoblastoma
|
|
Red Reflex |
|
The pinna of the ear usually joins the head above a horizontal line from the external canthus of the eye. A low-set ear suggests chromosomal anomaly and malformed ears are associated with renal abnormalities. Babies with Down Syndrome also may have small ears that fold over on top. However, a pre-auricular skin tag is usually of no significance.
The nose should be checked for patency by auscultation with a stethoscope. Babies are obligate nose breathers for the first few months of life and blockage of the nasal canal, or choanal atresia, can be life-threatening. The nose in Down Syndrome may be small, with a flattened nasal bridge.
A neonatal tooth is occasionally observed and usually requires extraction. The palate should be examined for the presence of a cleft. The neck should be checked for webbing, mass, or goiter. |
The respiratory rate in the newborn range is between 40 and 60 breaths/minute. Respiration might be periodic with short periods of apnea. There should be no nasal flaring or intercostal of subcostal retractions.
The breasts are palpable in term infants and may secrete a small amount of milk because of estrogenic effects from the mother (witch's milk). Unusually widely spaced nipples may be suggestive of a chromosomal anomaly.
The normal pulse rate of a newborn is 120 to 140 beats/minute. A persistent heart rate of less than 100 or more than 160 beats/minute is a cause for concern.
Absence of peripheral pulses, especially the femorals, suggests coarctation of the aorta.
Normal blood pressure is about 60/30 mm of Hg at term.
Transient murmurs are often heard after birth, but the presence of a loud murmur, heart sounds that are difficult to hear or are heard louder on the right side of the chest, or central cyanosis suggest a significant cardiac abnormality.
The umbilical cord should have two arteries and one vein. A single umbilical artery is seen in 1% of babies and is sometimes associated with other congenital anomalies.
Umbilical hernia is common and usually closes spontaneously before two years of age.
The liver normally extends 2 cm below the costal margin, and the tip of the spleen can sometimes be felt. Both kidneys can be palpated. Abnormal masses such as Wilm's tumor, neuroblastoma, hydronephrosis or a multicystic-dysplastic kidney or renal vein thrombosis can be easily palpated. A tight abdomen or persistent abdominal distention suggests intestinal obstruction or ascites.
The back should be checked for midline defects; a shallow sacral dimple is a common and normal finding. However, a deep dimple needs to be further investigated.
In the female infant, the vaginal opening is visible and a mucoid discharge, which might be bloody secondary to estrogen withdrawal, is not uncommon. The labia minora and clitoris are prominent, but in the term female, the labia majora cover the clitoris and the labia minora.
In the male newborn, the testes might not be fully descended at birth, especially if the baby is premature. Hydroceles and inguinal hernias are common. The prepuce adheres to the glans penis and should not be retracted. The meatus should be located at the tip of the penis.
Any apparent abnormality in the size or shape of the genitalia mandates a consultation with the pediatric urologist and/or endocrinologist.
|
Ambiguous Genitalia |
|
The anus should be checked for patency, position, and the anal reflex. |
Each extremity should be carefully examined for polydactyly or syndactyly. Most babies have three palmar creases. A single palmar crease crossing the hand is present in about 4% of normal babies but may also be associated with chromosomal anomalies such as Down Syndrome.
|
Single Palmar Crease |
Bowing of the legs is a normal variation, as are positional abnormalities such as metatarsus adductus which result from intrauterine compression, but one should be able to place the extremity easily in the normal position. Inability to do so suggests pathology.
Developmental hip dysplasia (congenital dislocation) occurs in 1-3/1000 live births. It is more common in females by a 9:1 ratio, and is more common in children who have been in a breech position in utero. Suspicion of hip dysplasia requires immediate consultation with a pediatric orthopedic surgeon.
To check for this condition, the baby should be placed supine with the hips and knees flexed to 90°. The middle finger of each hand is placed over the greater trochanter of the tibia and the thumb on the opposite side of the hip joint, over the lesser trochanter. First a posterior pressure is applied; if the hip is dislocatable, it will snap out of the acetabulum with a click or a clunk. However, if the head of the femur is already dislocated, abducting the hips will be difficult or will result in a click as the head of the femur slips forward into the acetabulum. These maneuvers can best be performed on both hips simultaneously or while stabilizing the other hip with the opposite hand.
|
More info: Evaluation |
|
Evaluation and Referral for Developmental Dysplasia of the Hip for Infants
|
Useful information can be gained simply by observing the baby's posture, alertness, and level of activity. A normal term baby lies flexed in the fetal position with the hands closed, whereas a premature baby sprawls out with the hands open.
 A normal baby is easily awakened by taking off the covers or by stimulating the foot or the cheek, while a depressed baby is poorly responsive and quickly goes back to sleep.
A normal baby is easily awakened by taking off the covers or by stimulating the foot or the cheek, while a depressed baby is poorly responsive and quickly goes back to sleep.
A full-term baby with decreased flexor tone and lying with the limbs extended may either be floppy or have increased extensor tone. This calls for immediate further evaluation for intracranial pathology, muscle disease, or a systemic disorder such as hypotension or infection.
Cranial nerves may quickly tested by eliciting the pupillary responses and blink reflex to light (II), doll's eye phenomenon (III, IV, VI), corneal, sucking, and rooting reflexes (V, VII), response to noise or sound (VIII), and the gag reflex (IX, X).
The integrity of the lower brain centers can be checked by eliciting the neonatal reflexes: Moro reflex, grasp reflex, sucking and rooting reflex, and the stepping reflex. In addition, the Moro reflex is useful in establishing that movements of the extremities are symmetrical.
![]()
At the time of discharge, the baby is re-examined and a postpartum outpatient visit is scheduled. The discharge examination is essentially similar to the one performed shortly after birth. The purpose is to:
|
More information on screening |
|
Screening from Savebabies.org Screening by State from babysfirsttest |
The clavicle is the bone most commonly fractured during labor and delivery. The fracture is usually of the "greenstick" variety, meaning that the fracture does not extend all the way through the bone. Crepitus and irregularity are present on palpation over the fracture. Active or passive movement of the arm is painful, and the Moro reflex is usually absent on the involved side. Therapy consists of immobilizing the arm and shoulder, usually for seven to 10 days, so as to minimize discomfort. Prognosis is excellent and complete healing should be expected in four to six weeks.
Skull fractures are uncommon and usually result from difficult delivery or forceps extraction. The fracture may be linear or depressed. Linear fractures are accompanied by soft tissue swelling. A depressed fracture usually results in a visible and palpable indentation. Most fractures are asymptomatic but fractures that are associated with the neurological symptoms may require surgical elevation of the depressed segment.
Petechiae found on the head, neck, chest, and back because of difficult delivery are not progressive. In contrast, petechiae resulting from hemorrhagic disorders are generally progressive and are distributed all over the body. Bruises and ecchymoses may also be seen after a difficult delivery. Hyperbilirubinemia may result from breakdown of the extravasated blood.
Cephalohematoma is a subperiosteal collection of blood resulting from traumatic rupture of blood vessels passing from the skull to the periosteum. Cephalohematoma is most common over the parietal bone and does not cross suture lines in contrast to the edema of caput succedaneum. Significant blood loss and a linear skull fracture may be associated with a cephalohematoma. Incision or aspiration of a cephalohematoma is contraindicated because of the risk of infection. By three to four days of age, the area is fluctuant and has a peripheral edge of organizing tissue. Most cephalohematoma are re-absorbed in two to three months.
Brachial plexus injury results from trauma to one or more of the spinal roots C5 to C8 during birth. The arm is held adducted with internal rotation, extension at the elbow, pronation of the forearm and flexion at the wrist.
Muscle tone is decreased and reflexes are absent. If the nerve roots are intact, most infants recover from this injury within three to six months. Physical therapy should be provided to maintain the range of motion.
Hyperextension of the neck during delivery can result in phrenic nerve injury (C3 to C5) and diaphragmatic paralysis. The infant develops respiratory distress and often has an associated brachial plexus injury. Most infants recover spontaneously within two to 3 months.
![]()
HIE results from inadequate oxygen supply to the brain and is a major cause of perinatal death and subsequent neurological disability. Ideally, personnel skilled in neonatal resuscitation should be present at every high-risk delivery.
In the newborn period, HIE is associated most often with diminished fetal oxygenation due to perinatal events, though it can also result from severe cardiovascular or pulmonary insufficiency in the neonatal period. The fetus may be subject to intrauterine hypoxia due to uteroplacental insufficiency with reduced oxygen delivery to the fetus. Conditions such as abruptio placentae, maternal hypertension, or having the umbilical cord wrapped around the neck may increase the risk of oxygen deprivation.
In practical terms, neonatal encephalopathy due to hypoxia or ischemia is a greater risk in babies with a 5-minute Apgar score of 0 to 3 and with an arterial pH of 7 or less. Complications include neurological injury but also cardiac, renal, intestinal, and hepatic damage. Neurological damage may be reduced in the full-term baby by immediately instituting hypothermic management for the first 72 hours of life.
Jaundice is seen in approximately half of all newborns. Although neonatal hyperbilirubinemia is usually a benign and physiologic condition, very high bilirubin levels occur in certain pathologic conditions and are potentially injurious to the central nervous system.
Bilirubin is a product of heme catabolism. Red cell hemoglobin accounts for approximately 85% of all bilirubin. In newborns, the normal hemoglobin level is 15-18 mg/dl. The rate of neonatal RBC destruction is higher than in adults resulting in greater quantity of hemoglobin release. Excessive bruising from birth trauma or abnormal blood collections such as in a cephalohematoma may further add to the rate of RBC destruction and bilirubin formation.
Heme is catabolized to unconjugated bilirubin in the reticuloendothelial system. Unconjugated bilirubin is bound to albumin in the plasma and transported bound to albumin to the liver and is conjugated with glucuronic acid in the hepatocytes; the conjugation is catalyzed by glucuronyl transferase. Conjugated bilirubin is secreted into the bile and enters the duodenum. In the small bowel, some of the bilirubin is hydrolyzed to yield unconjugated bilirubin and glucuronic acid. Most unconjugated bilirubin is excreted in the stool, but some is reabsorbed and returned to the liver for re-conjugation (enterohepatic circulation).
The level of glucuronyl transferase is initially low in the newborn and any increase in the rate of bilirubin formation can overwhelm the capacity to conjugate, thus resulting in elevated bilirubin levels.
When the serum level of unconjugated bilirubin exceeds the albumin binding capacity, bilirubin diffuses into the central nervous system and may result in permanent neurological damage or death (bilirubin encephalopathy with kernicterus).
Conjugated bilirubin is water soluble and does not diffuse into the central nervous system so it is not capable of causing kernicterus.
Factors such as acidosis and hypoalbuminemia may reduce the ability of albumin to bind to conjugated bilirubin. The specific serum level of unconjugated bilirubin that results in kernicterus is unknown, but for the term infant it has traditionally been defined as a concentration of 20 mg/dl. In the low birthweight infant, the level is proportionately lower.
|
More information on Jaundice |
|
Bilirubin metabolism from Merck Kernicterus from eMedicine
|
The most common cause of neonatal jaundice is physiologic hyperbilirubinemia.
In the term infant, physiologic hyperbilirubinemia appears at about two days of age, peaks at 10 to 12 mg/dl at three to four days and disappears by four to seven days. Low birthweight infants have exaggerated and prolonged physiologic hyperbilirubinemia, which may persist for 10 to 14 days.
The following scenarios suggest pathologic hyperbilirubinemia:
Pathologic hyperbilirubinemia may result from overproduction or under-secretion of bilirubin, or sometimes from a combination of the two.
Clues to the etiology of neonatal hyperbilirubinemia may be obtained by reviewing the family, maternal, and neonatal history. Clues are also found in the course of jaundice.
Excessive hemolysis with overproduction of bilirubin is the most common cause of neonatal hyperbilirubinemia. Jaundice that appears early suggests abnormally rapid destruction of red blood cells. Hemolytic disease in the newborn has two common causes:
Infants with ABO or Rh incompatibility may have anemia or progressively falling HCT with reticulocytosis. The direct Coombs test is usually positive.
Less frequently, neonatal hyperbilirubinemia may result from a inherited hemolytic disorder such as hereditary spherocytosis, glucose-6-phosphate dehydrogenase deficiency or a hemoglobinopathy such as thalassemia.
Infants with a cephalohematoma or excessive bruising may develop hyperbilirubinemia from breakdown of the extravasated blood. Similarly, the infant with an unusually high HCT (venous HCT >65%) may have hyperbilirubinemia from the normal rate of destruction of an abnormally large red cell mass.
Hyperbilirubinemia may also result from increased enterohepatic circulation of bilirubin from delayed passage of meconium resulting from mechanical obstruction or reduced peristalsis.
|
More information on Jaundice |
|
Hemolytic disease of the newborn
|
These are uncommon and result from biliary obstruction or the impairment of hepatic uptake, conjugation, or canalicular transport of bilirubin. The hyperbilirubinemia may be unconjugated or conjugated, depending on whether the etiology is inadequate conjugation or inadequate biliary secretion. Examples include metabolic disorders such as Crigler-Najar syndrome (unconjugated), galactosemia and biliary atresia (conjugated). This type of disorder should be suspected if jaundice is prolonged beyond the first week of life.
These include bacterial sepsis, intrauterine infections such as syphilis, and metabolic disorders such as maternal diabetes mellitus. Note also that babies who are exclusively breastfed may have an exaggerated course of physiologic jaundice possibly related to increased enterohepatic recirculation of bilirubin.
With a serum bilirubin level of around 5 mg/dl, jaundice appears on the face. Jaundice proceeds caudally as the bilirubin level increases. The physical examination should be performed looking for extravascular collections of blood such as a cephalohematoma or for hepatosplenomegaly which is found in infection and hemolytic anemia. Petechiae suggest intrauterine infection, sepsis, or severe hemolytic disease. Lethargy, poor feeding, and temperature instability may indicate sepsis.
The following initial laboratory studies should be obtained in any infant who appears to have pathological jaundice:
The goal of management is to prevent bilirubin encephalopathy or kernicterus.
|
More information on managing jaundice |
|
Management of neonatal jaundice from eMedicine
|
It is very important to determine the baby's age in hours at the time of assessment and his/her risk factors for severe hyperbilirubinemia.
An excellent reference for this process is Bilitool from Bilitool.org
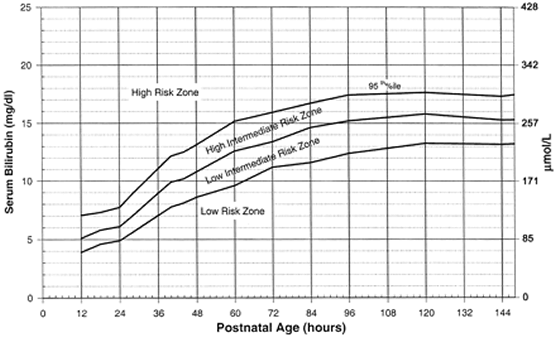
The Bhutani Nomogram is used to determine the level of risk based on the Infant's hours of age and serum bilirubin result.
Major Risk Factors for severe hyperbilirubinemia in infants >35 weeks gestational age:
Guidelines for phototherapy based on infant's age, risk factors, and serum bilirubin help us determine the course of action.
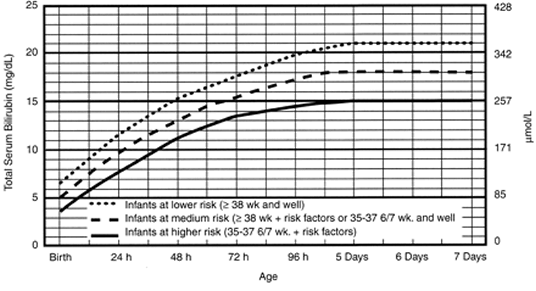
![]()
Bhutani, Vinod K., Lois Johnson, and Emidio M. Sivieri. "Predictive ability of a predischarge hour-specific serum bilirubin for subsequent significant hyperbilirubinemia in healthy term and near-term newborns." Pediatrics 103.1 (1999): 6-14.
Respiratory disease is a common cause of neonatal morbidity.
The etiology of this condition is thought to be delayed resorption of fetal lung fluid. This condition is more common in term infants, especially those delivered by cesarean section. The symptoms consist of tachypnea, grunting, and nasal flaring. The infant might display cyanosis. Most infants recover within 12 to 24 hours, though the symptoms may last as long as three days. Oxygen therapy is usually required for a few hours. Radiographic examination reveals central perihilar streaking and fluid in the fissures.
Meconium staining is seen in about 10% of all pregnancies and almost half of post-date pregnancies and may result from intrauterine fetal distress. The aspiration of meconium- stained amniotic fluid results in severe respiratory distress. The thick material produces a ball-valve effect with areas of over- expansion and atelectasis. Pneumothorax is a frequent complication in the over-expanded areas of the lung. Oxygenation and ventilation are compromised, and persistent pulmonary hypertension might result.
RDS results from the inability of the premature infant to synthesize pulmonary surfactant (surface-active lecithin). Surfactant is essential to reduce alveolar surface tension and keep the alveoli open during expiration. The hallmark of RDS is diffuse atelectasis.
RDS is uncommon in the term infant. The more premature the infant, the more likely the development of RDS. In addition to prematurity, the risk for RDS is increased by conditions that delay lung maturity such as maternal diabetes, male sex, and Caucasian race. Conversely, lung maturity can be hastened by the stress of intrauterine growth retardation and also by administration of antenatal glucocorticoids to the mother.
The infant with RDS displays tachypnea, retractions, nasal flaring, grunting, and cyanosis within a few hours of birth. The chest radiograph demonstrates a reticulo-granular "ground-glass" appearance with air bronchograms.
Administration of oxygen, artificial surfactant and respiratory support are the keystones of management.
In the fetus, glucose is supplied via the placenta. Following birth, maternal glucose is no longer available and the newborn must maintain the blood glucose level by glycogenolysis or lipolysis.
After birth, the blood glucose level declines to a minimum of 35 mg/dl and by four to six hours it stabilizes at approximately 50 to 60 mg/dl. Neonatal hypoglycemia within the first 72 hours is defined as plasma glucose of less than 40 mg/dl. After 72 hours of life, 45 mg/dl is the lower limit of normal. Plasma glucose values are approximately 5 mg/dl higher than the whole blood values (chem-strip; dextrostix).
Infants of diabetic mothers are particularly prone to hypoglycemia because of persistent endogenous hyperinsulinemia in response to maternal hyperglycemia. These infants are often LGA with a birth weight exceeding 4 kg. Conversely, SGA infants have often had intrauterine malnutrition. Such infants are also prone to hypoglycemia because of inadequate nutritional reserves. Hypoglycemia is also common in the smaller of discordant twins. Infants with hypoxic ischemic encephalopathy have an increased energy expenditure and are also susceptible to hypoglycemia.
Symptoms of hypoglycemia include jitteriness, seizures, cyanosis, apnea, hypotonia, and poor feeding. Some infants may be completely asymptomatic.
Rapid bedside determination of whole blood glucose concentration can be performed with a test-strip such as Glucostix(r) or Chemstrip(r). A low value must immediately be confirmed by laboratory determination.
Treatment and prognosis: the best therapy is prevention. In an infant with a falling blood glucose level, early feedings, either enteral or parenteral should be initiated. Intravenous infusion of 10% dextrose in water to provide a glucose delivery rate of 5 to 8 mg/kg/min is generally adequate in an infant who cannot be fed enterally.
![]()
Use of drugs during pregnancy can have profound effects upon the fetus.
Heroin: miscarriage, abruptio placentae, prematurity, SGA; withdrawal symptoms including irritability, continual crying, jitteriness, vomiting, sneezing.
Methadone: withdrawal symptoms including seizures.
Cocaine: prematurity, SGA, smaller head circumference, abruptio placentae, abnormal sleeping pattern, irritability, and possibly urinary tract abnormalities.
Ecstasy and other amphetamines: possible heart defects and cleft palate.
|
More information on substancy abuse during pregnancy |
|
Illicit drug use during pregnancy from March of Dimes
|
Neonatal sepsis is defined as a positive blood culture during the first 28 days of life. Infection is most commonly caused by organisms present in the birth canal, though it may also be acquired by the transplacental route or from an environmental pathogen following birth. The most common organisms are group B beta-hemolytic streptococci, and E. coli. Other enteric bacteria, Listeria and Staphylococcus aureus may also be implicated. Premature babies are also at risk for infection with coagulase negative staphylococci and Candida.
The physician should be especially alert to the possibility of neonatal sepsis when the maternal history indicates cervical colonization with potentially infectious organisms such as group B streptococci, prolonged rupture of the membranes, or chorioamnionitis.
The signs and symptoms of neonatal sepsis may be subtle. The baby may just be "not doing well", or may exhibit fever, hypothermia, poor feeding, jaundice, abdominal distention, vomiting, apnea, irritability, or pallor or mottling.
Cultures must be obtained of blood, urine (by steile catheterization or suprapubic aspiration) and cerebrospinal fluid. A positive culture confirms the diagnosis of sepsis, but the negative culture does not necessarily exclude it.
Because meningitis occurs in a significant proportion of septic neonates, the cerebrospinal fluid should also be sent for cell count, Gram stain, culture and protein and glucose determination. CBC and chest x-ray are generally also obtained and may provide a clue to the presence or site of infection.
Treatment must be initiated as soon as sepsis is suspected, even before results of cultures and diagnostic studies have been determined. Initial therapy should include broad-spectrum antibiotic coverage. A combination of ampicillin and gentamicin is the usual initial regimen. Once the organism and its antibiotic sensitivity pattern have been identified, the single most effective antibiotic should be continued for 7 to 10 days. Meningitis needs to be treated for two to three weeks.
Congenital infections are usually acquired by transplacental entry of the organism from the mother's bloodstream into the fetus, though infection may also occur during passage through the birth canal. The acronym TORCH is commonly used to list infections caused by Toxoplasmosis, Other (syphilis, varicella zoster, parvovirus) Rubella, Cytomegalovirus and Herpes simplex.
Transplacentally acquired infections may result in fetal loss, intrauterine growth retardation, prematurity, or postnatal disease. Following birth, congenitally acquired infections may present as central nervous system abnormalities such as microcephaly; hepatosplenomegaly with abnormal liver function tests, and thrombocytopenia. Each of the infecting agents also produces its own characteristic clinical features:
Toxoplasmosis: chorioretinitis, obstructive hydrocephalus, mental retardation, intracranial calcification, and convulsions. The infection may not be obvious at birth.
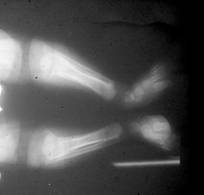
Syphilis: hepatosplenomegaly, nasal discharge or "sniffles", anemia, thrombocytopenia, mucocutaneous rash, periosteitis, osteochondritis, nephrotic syndrome, and central nervous system abnormalities.
|
Syphilis with Periostitis |
Rubella: hepatosplenomegaly, growth retardation, thrombocytopenia, petechiae, "blueberry muffin" lesions. Late features include deafness, cataracts, and mental retardation.
Cytomegalovirus: CNS abnormalities, hepatosplenomegaly, and intracranial calcifications. Deafness in later life is an important complication and may be the only clinical manifestation.
Herpes simplex: vesicles, encephalitis, or disseminated infection with multi-organ failure. Congenital herpes simplex is a medical emergency. Most neonate infections due to herpes simplex are not present at birth. Rather, the disease is acquired by direct contact during delivery to a mother who is infected. The incubation period is about 5 to 10 days and the baby presents with cutaneous lesions and/or systemic signs and symptoms suggesting sepsis.
|
Herpes Vesicles |
Human immunodeficiency virus: HIV infection may be acquired transplacentally, by exposure to blood during delivery, or via breast milk. Infection occurs in approximately 25% of the exposed children. Medication and careful perinatal management reduces the transmission rate in the US to about 2%. Treatment of the mother and subsequently the child with zidovudine significantly reduces the risk of infection.
Parvovirus B19 infection in the fetus can cause intrauterine anemia leading to congestive cardiac failure and hydrops fetalis. Varicella zoster infection may lead to cutaneous scarring, atrophy of the extremities, microcephaly, mental retardation, cataracts, and abnormalities of bladder and bowel function.
![]()
APGAR from NLM
Ballard Score from Medcalc
Bilirubin metabolism from Merck
Breast feeding common concerns
Breast or Bottle? From Kidshealth
Circumcision: AAP Policy
Hemolytic disease of the newborn
Hemorrhagic disease from Lucile Packard Children's Hospital
Evaluation and Referral for Developmental Dysplasia of the Hip for Infants
Illicit drug use during pregnancy from March of Dimes
Jaundice (neonatal) management from eMedicine
Kernicterus from eMedicine
Mnemonics and Greek mythology