Musculoskeletal Injuries
A Chapter in Core Concepts of Pediatrics, 2nd Edition
Sharon Sanchez, MD; Tamantha Arlata, MD; Saima Arshad, MD; Sarah Cheng, MD; Andrea Saunders, MD
Musculoskeletal injury is one of the most common reasons for visiting a pediatric urgent care setting. Accidental injuries occur frequently during recreational play for toddlers and early school-aged children and more commonly during organized sports for older children. As organized sports participation increases for younger children, the prevalence of musculoskeletal-related injuries from athletic participation is shifting downward for age.
This chapter outlines common injuries, evaluations, and management strategies for pediatric patients, including children and adolescents. It is important to understand that bone structure, musculature, and joint stability differ between the pediatric and adult populations. While most pediatric musculoskeletal injuries can be managed by pediatric primary/urgent care providers, having a collaborative relationship with the orthopedic specialists is advantageous.
Fractures
Physical Examination
Evaluation: Imaging
Anteroposterior (AP) and lateral views are the most common.
Oblique views are helpful for fully disclosing the nature and extent of many fracture patterns, especially when the injury involves the ankle, elbow, hand (especially for scaphoid fracture), or foot. Oblique views are also helpful for detecting subtle spiral fractures where the AP and lateral views are normal, yet a fracture is strongly suspected.
Ankle AP mortise view is helpful since it includes distal tibia, distal fibula, talus, and proximal metatarsals.
This is the standard classification system for description of fractures involving the growth plate (also called physis or epiphyseal plate).
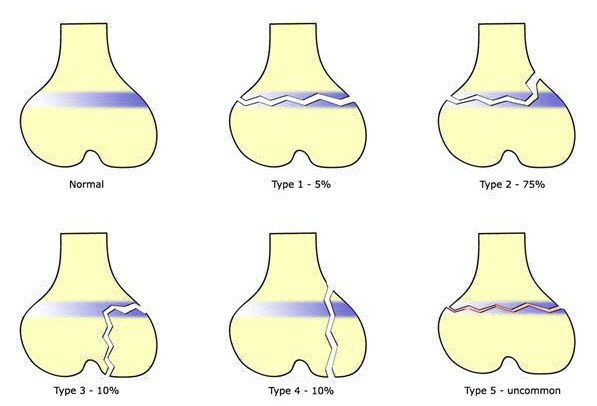
Prevalence of Fracture Types Using the Salter-Harris Classification System
|
Type I Fracture through physis; extra-articular |
||
|---|---|---|
|
Salter-Harris Type I on right distal tibia |
Salter-Harris Type I on right proximal tibia |
Salter-Harris Type I on left distal radial |
|
Type II Fracture through physis and metaphysis |
||
|
|
Salter-Harris Type II on distal femur |
|
|
Type III Fracture through epiphysis and physis |
||
|
Salter-Harris Type III on distal tibia |
Salter-Harris Type III on right distal tibia |
|
|
Type IV Fracture through epiphysis, physis, and metaphysis |
||
|
|
Salter-Harris Type IV of base of proximal phalanx |
|
|
Type V Compression injury to physis without fracture. Rare and identifiable only in retrospect, when compression of the physis has led to growth disturbance. |
||
|
Salter-Harris Type V on distal tibia |
Salter-Harris V through medial aspect of left distal tibia
|
|
Mechanism of Injury
The Mechanism of Injury is blunt trauma or indirect trauma (including overuse injury in throwers such as Little Leaguers shoulder.
Radiographs show mild widening of the physis and metaphyseal changes


Proximal humerus fracture
1b. Humerus shaft fracture
Mechanism of Injury
Often associated with trauma. Consider non-accidental trauma if less than three years of age and spiral fracture pattern.

Humerus shaft fracture
Supracondylar fractures represent half of pediatric elbow fractures and most operated pediatric fracture.
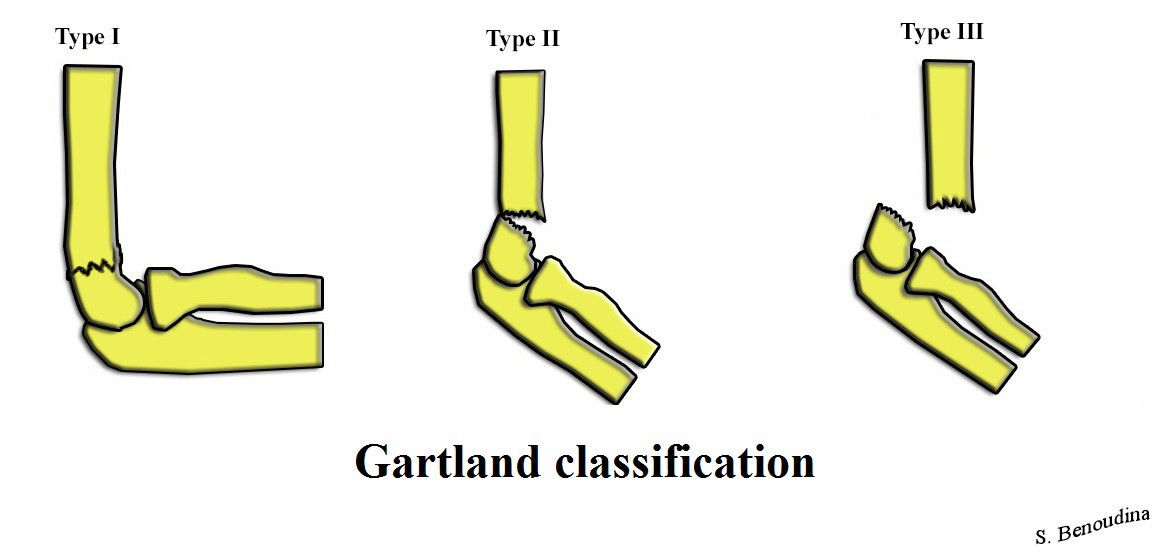
Gartland Classification of Supracondylar Humerus Fracture
Image Source from Wikimedia Commons: https://upload.wikimedia.org/Wikimedia/commons/f/fc/Gartland_Classification.jpg
Mechanism of Injury
Associated Injuries
Radial nerve palsy is the second most common neuropraxia. On exam, patient is unable to extend wrist or digits.
Ulnar nerve palsy is seen with flexion-type injury patterns.
Evaluation: Imaging
AP and lateral view of the elbow x-rays show posterior fat pad sign : lucency along the posterior distal humerus and olecranon fossa is highly suggestive of occult fracture around the elbow.

Supracondylar humerus fracture

Supracondylar humerus fracture


Supracondylar humerus fracture
Management
2b. Medial epicondyle fracture
Mechanism of Injury
Injury can be a fall on an outstretched arm (most common), elbow dislocation, traumatic avulsion (usually occurs in overhead throwing).
Medial epicondyle fracture
Physical Examination
Tenderness over medial epicondyle.
2c. Lateral condyle fracture
Medial epicondyle fracture
Mechanism of Injury
Results from the pull of the common extensor musculature or fall on an outstretched hand.
Physical Examination
Swelling and tenderness to the lateral elbow is notable on exam. There is also increased pain upon wrist extension or flexion.
2d. Radial head / neck fractures (of the elbow)
Mechanism of Injury
Typically involves valgus loading injury of the elbow.
Physical Examination
There is swelling over lateral elbow. Pain is exacerbated upon forearm supination and pronation. Sometimes, there is referred pain to the wrist.
Radial head/neck fractures
Apex volar (Colles' fracture)
Apex dorsal (Smith's fracture)
3b. Distal metaphysis (incomplete fracture)
Torus/Buckle fracture (typically unicortical)
3c. Diaphysis
Plastic deformation: incomplete fracture with deforming force resulting in shape change of bone without clear fracture line, occurs along compression side.
Greenstick fracture: incomplete fracture resulting from failure along tension (convex) side.
Buckle /Torus fracture of the dorsolateral cortex of the distal radial metaphysis

Plastic deformation (bowing deformity) of the right radius
and an oblique mid-diaphyseal ulnar fracture
with posterior displacement of the distal fragment (one shaft-width)
Abuse must be considered if child is less than five years of age, especially if present in a patient before walking age. Femur fractures are the second most common child abuse associated fracture after humerus fractures. (See also the section below on Non-accidental fractures.)
Symptoms
Patients typically present with thigh pain, inability to walk, report of leg deformity or instability.
Mechanism of Injury
The mechanisms of injury is correlated with age due to the increasing thickness of the cortical shaft during skeletal growth and maturity. Falls are the most common cause in toddlers. Whereas, high energy trauma is responsible for injury in adolescents, typically from motor vehicle collision. Fractures after minor trauma can be the result of a pathologic process (bone tumors, osteogenesis imperfecta, osteopenia).
Physical Examination
Examination reveals gross deformity, swelling of the thigh, and exquisite tenderness to affected area.
Evaluation: Imaging
X-rays:
Management
Complications
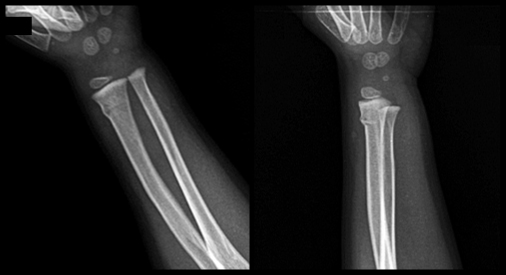
This type of fracture is also referred to as childhood accidental spiral tibial (CAST) fractures
Mechanism of Injury
The injury is low energy trauma with rotational component or hyperextension of the knee when landing from a jump.
Physical Examination
Child may limp or refuse to walk. Exam shows tenderness but no obvious swelling or deformity.
Evaluation: Imaging
X-ray may reveal nondisplaced spiral or oblique fracture (distal metaphyseal oblique proximal lateral to distal medial) of tibial shaft only. Fibula typically remains intact. Toddler fracture involves the distal half of tibia, unlike non-accidental injury, which typically involves proximal half of tibia.
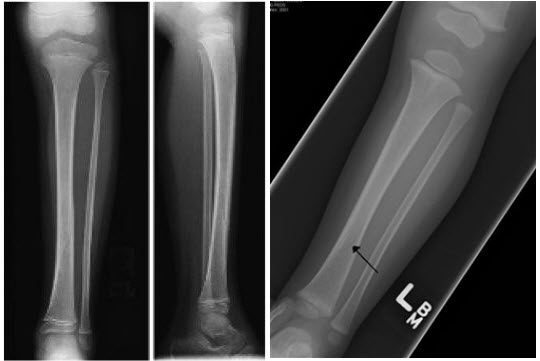
Tibia shaft fracture (Toddler fracture)
Stress fractures most commonly affect the long bones of the lower legs (more commonly the tibia) but can also involve the foot, hip, knee, or ankle.
Mechanism of Injury
Overuse injuries commonly cause abnormal stresses on trabecular bone resulting in microfractures, which subsequently propagates within the bone. Repetitive loads then exceed the threshold of intrinsic bone healing. This is commonly seen in young athletes.
Evaluation: Imaging
X-ray may be normal. Sometimes, injuries require bone scan to confirm diagnosis.

Stress Fracture
Mechanism of Injury
Most commonly via axial load across hyper-extended and radially deviated wrist.
Physical Examination:
Evaluation: Imaging
Management

Scaphoid Fracture
Mechanism of Injury
Trauma, including sports, is the most common cause of injury.
Physical Examination
Examination reveals localized tenderness and/or deformity. Look carefully for open wounds.
Evaluation: Imaging
Finger X-ray: Obtain AP and lateral views if there is a specific, localized area of pain.
Hand X-ray: Obtain hand x-ray if there are suspicion for carpal or metacarpal bone involvement.

Spiral Fracture on proximal phalanx of 2nd digit
Management
Goals of splinting
Equipment
|
TYPES OF SPLINTS |
|
|---|---|
|
Splints for |
Indication |
|
Bulky hand compression dressing |
Closed hand fractures |
|
Colles splint |
Distal forearm and wrist fractures |
|
Dorsal or volar splint |
Wrist fractures or injuries, fractures of 2nd - 5th metacarpals, soft tissue injuries of the hand |
|
Figure-of-eight splint |
Medial clavical fractures |
|
Gutter splint |
Phalangeal and metacarpal fractures |
|
Posterior arm splint |
Stable elbow and forearm injuries |
|
Sling and swathe |
Shoulder injuries, humeral injuries |
|
Sugar tong splints |
|
|
Proximal |
Humeral fractures |
|
Distal |
Wrist fractures, distal forearm fractures |
|
Double |
Elbow fractures, forearm fractures |
|
Reverse |
Distal forearm fractures |
|
Thumb spica splint |
Scaphoid fractures, extra-articular fractures of the thumb metacarpal, ulnar collateral ligament injuries |
|
Velpeau bandage |
Shoulder injuries, humeral injuries |
|
Volar finger splint |
Fractures of distal phalanges and interphalangeal joints |
|
Splints for |
Indication |
|
Buddy taping |
Phalangeal fractures of the toes |
|
Bulky foot compression dressing |
Calcaneal fractures; foot injuries |
|
Jones compression E |
Knee and calf injuries |
|
Knee splint |
Knee injuries |
|
Posterior ankle splint |
Distal leg, ankle, tarsal, and metatarsal fractures; reduced dislocations; severe sprains |
|
Stirrup splint |
Ankle fractures |
Applying a Distal Sugar Tong Splint
a 7 minute video by S. Sanchez, UTMB
The muscle groups are divided in compartments and bound by rigid fascial membranes. Compartment syndrome occurs when increased pressure within a closed fascial compartment (often due to bleeding and edema collection) causes neurovascular compromise and muscle ischemia. Increased pressure, exacerbated by capillary leaking, first occludes venous outflow and only later occludes arterial flow to produce the classic signs and symptoms. Compartment syndrome is defined as pressure greater or equal to 30 mm Hg.
Symptoms: paresthesia and intense pain (aggravated by passive stretching of the muscles).
Signs: affected area is swollen & tense, pallor, and decreased pulses.
Common fractures prone to compartment syndrome
Fractures may cause penetrating injuries to surrounding structures. Any overlying bony structures, if bloody and fatty exudate is oozing, usually reflect communication with the medullary cavity of a fractured bone.
In the knee joints, if serous or serosanguineous fluid flows during knee movement, this is suggestive of a penetration of the joint capsule. Air seen in the radiograph of the knee joint confirms the diagnosis. Absence does not rule out capsular penetration, but warrants exploration in the OR.
Neuropraxia is a type of peripheral nerve injury that is classified as a transient conduction block of motor or sensory function. Although nerve degeneration does not occur, there can be a loss of motor function. Patients are usually able to fully recover within a period of weeks to months.
Although vascular injury can occur, there is rich collateral circulation that can maintain circulation.
Fractures associated with neurovascular injury include:
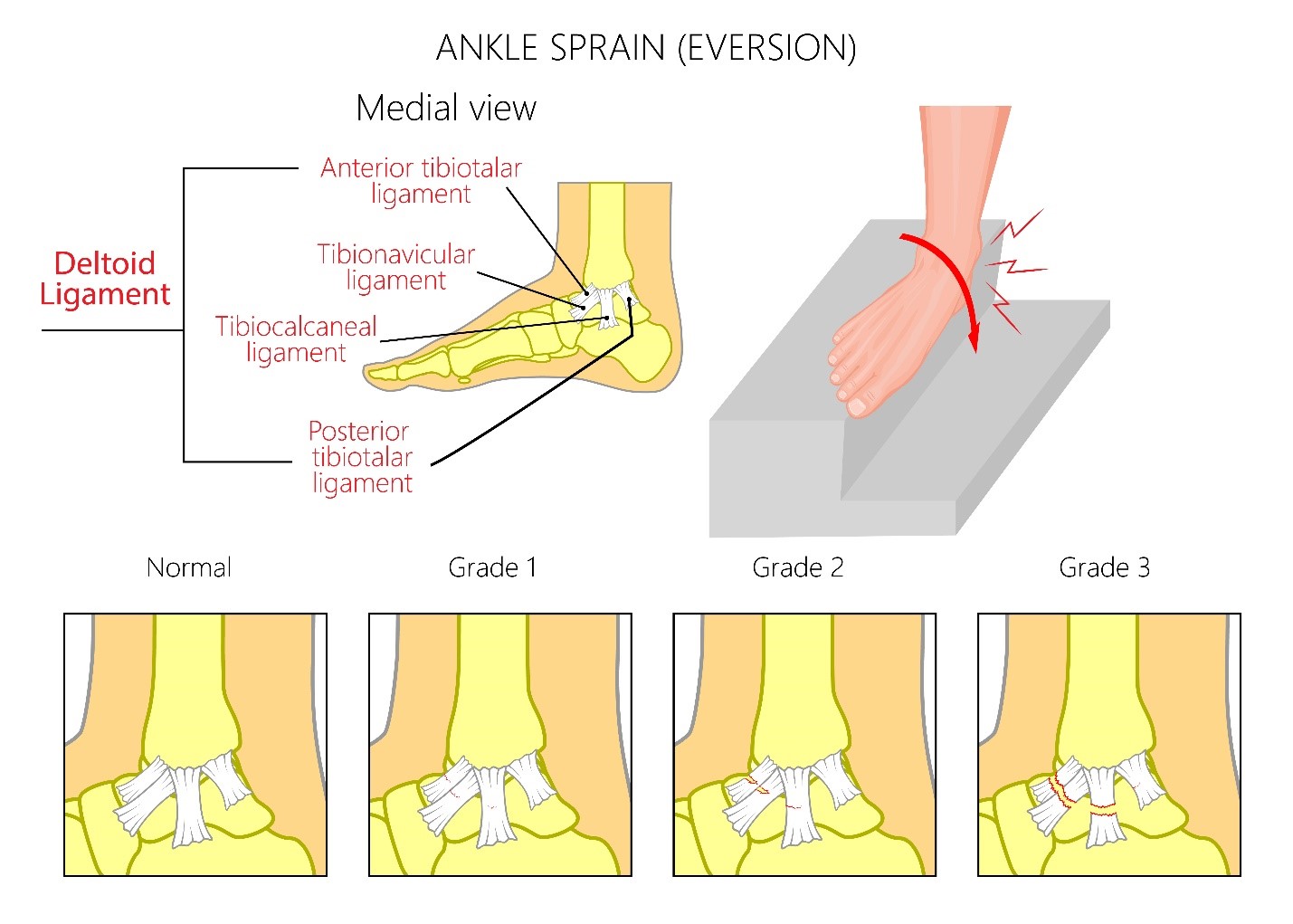
Sprains
A sprain is an injury to a ligament which is a band of short, fibrous connective tissue that connects between two bones or bone to cartilage to stabilize a joint together with other ligaments.
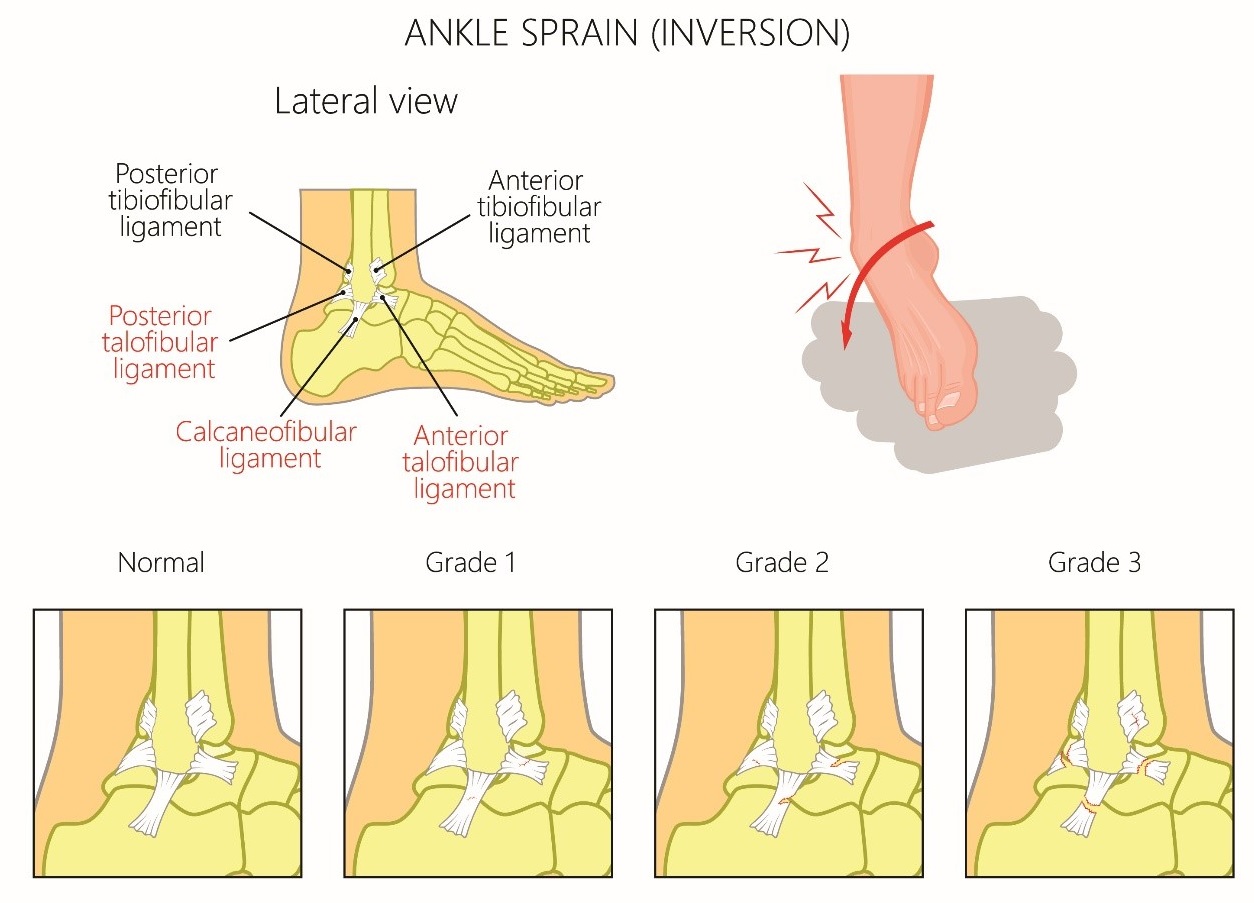
|
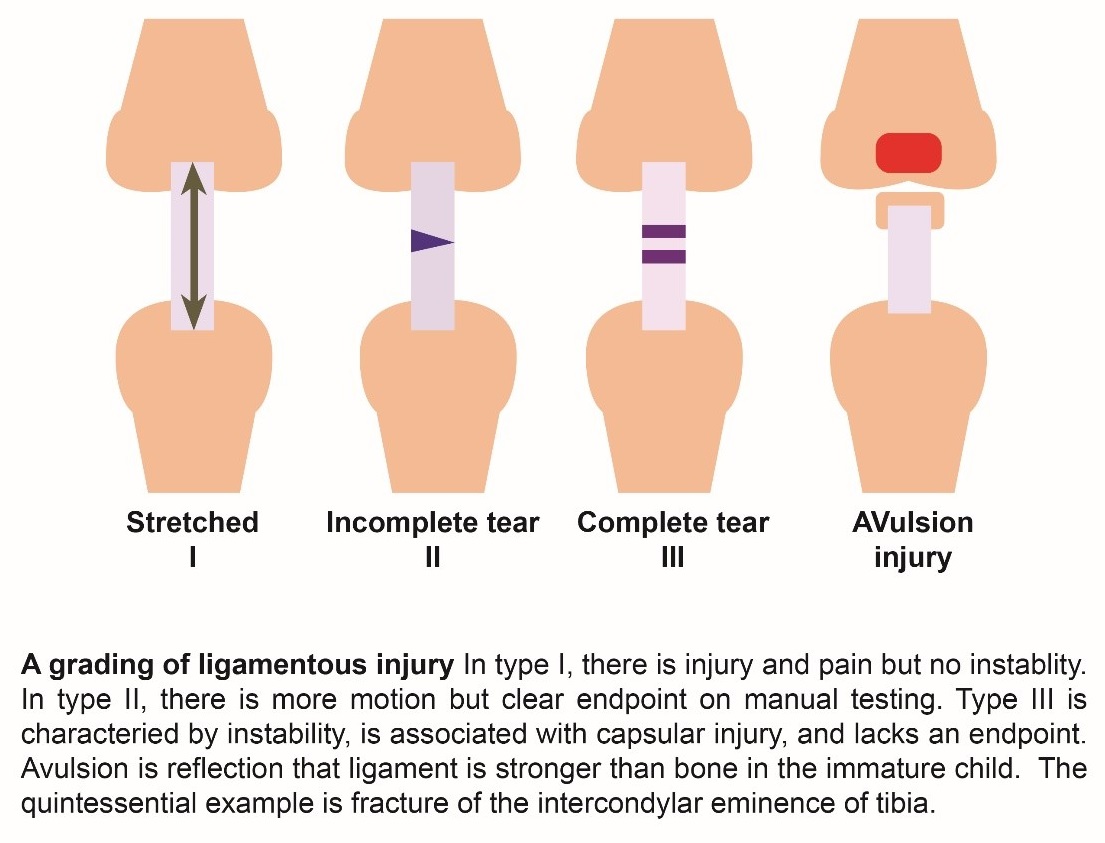
Sprain Severity Grading System Note that the time for healing of a sprain is not always proportional to the grade of the spran. |
|---|
|
Grade I sprain a. Mild stretching of a ligament with no or microscopic tears b. Mild tissue swelling and tenderness c. No joint instability or laxity on examination d. Able to bear weight and ambulate with minimal pain |
|
Grade II sprain a. An incomplete tear of a ligament b. Moderate pain, with soft tissue swelling, an effusion tenderness, and ecchymosis c. Mild to moderate joint instability with some restriction of the range of motion and loss of function d. Painful weight bearing and ambulation e. Require external support such as a brace or splint |
|
Grade III sprain a. A complete tear of a ligament b. Severe pain, swelling, tenderness, and ecchymosis c. Significant mechanical instability and loss of function and motion on examination d. Unable to bear weight or ambulate e. May require prolong external support for healing or sometimes surgery |
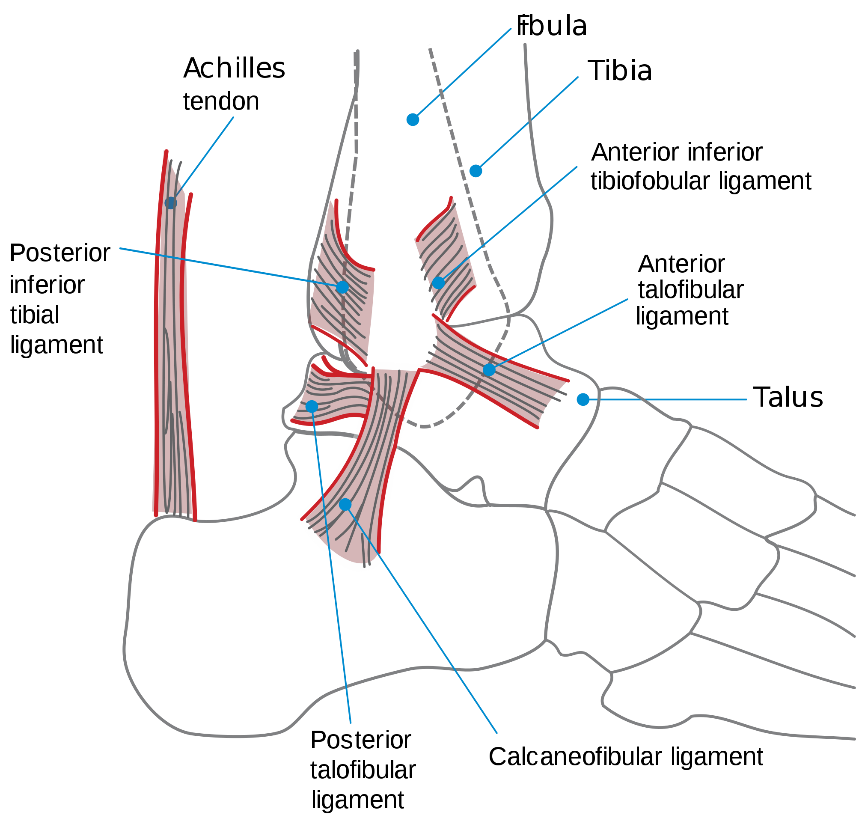
Image source from Wikimedia Commons: https://commons.wikimedia.org/wiki/File:Ankle_en.svg
Mechanism of Injury
Physical Examination
Physical exam should start with an inspection for swelling, ecchymosis and tenderness in the areas required for the Ottawa ankle rules (discussed below), and laxity of ankle ligaments, assessment for effusion, evaluation of range of motion including ambulation and neurovascular status, and comparison of the injured with the uninjured side.
Anterior Drawer Test
The test assesses the integrity of the ATFL. An examiner holds the lower leg with one hand and, while gripping the heel with the other hand, pulls anteriorly. Anterior displacement of the heel beneath the ankle in comparison with the contralateral side indicates a tear of the ATFL.
Talar Tilt Test
Inversion of the heel assesses the stability of the CFL. Eversion of the heel to assesses the integrity of the deltoid ligament.

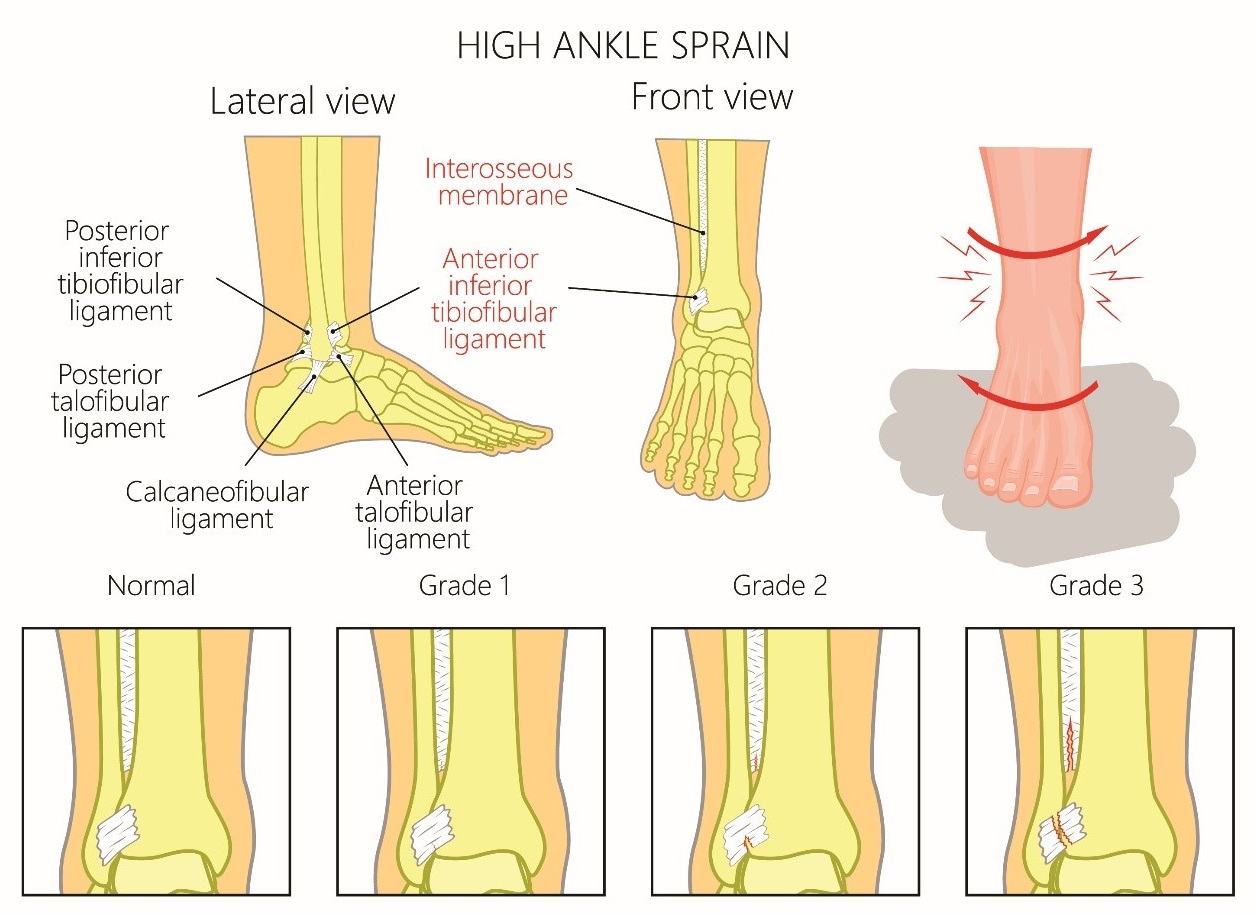
Tibia-Fibula Squeeze Test
The test identifies a syndesmotic sprain. It is a positive test when there is pain anterior and proximal to the ankle joint upon squeezing the tibia against the fibula at mid-calf. An orthopedist should be consulted for a syndesmotic sprain because surgery may be needed to maintain joint integrity and stability.
External Rotation Stress Test
This test also identifies a syndesmotic sprain. It is a positive test if pain is elicited in the region of the ATFL when the clinician stabilizes the leg proximal to the ankle joint, while grasping the plantar aspect of the foot and rotating the foot externally relative to the tibia.

Evaluation: Imaging
|
Ottawa Ankle Rules were created to limit unnecessary radiographs and are sensitive in children older than six years of age. An ankle series is recommended only if: Pain in the malleolar zone AND bony tenderness at the posterior edge or tip of the lateral or medial malleolus OR |
X-rays: in children, ligaments are stronger relative to their bones, and may need to rule out an underlying fracture first by radiography which should include antero-posterior, lateral, and oblique views.
A foot series is recommended only if there is pain in mid-foot zone AND any of the following findings:
Computed tomography may be used to rule out occult fracture.
MRI may be required for ankle pain not resolved after 6-8 weeks.
Management
a. Immobilization
Grade I sprain: An elastic (ace) wrap for a few days
Grade II sprain: The combination of an elastic wrap and an aircast for up to a few weeks
Grade III sprain: Ankle splints or below the knee cast for a brief period of immobilization followed by functional rehabilitation with gradual increase intensity by physical therapy
Referral to the orthopedist is beneficial, since surgery is sometimes considered in some patients with repeated large stresses on ankle joints.
b. Supportive Care: Immediate therapy - "RICE" treatment for the first two to three days
Rest: avoid movements/activities that can reproduce pain, use crutches.
Ice: apply on the affected area every 2-3 hours for 15-20 minutes each time for the first 48 hours or until swelling is improved. Place thin towel between the ice and skin.
Compression: wrap the affected joint with an elastic bandage to help support the joint and minimize swelling.
Elevation: raise the affected joint above the level of the heart.
c. Pain Control - Nonsteroidal anti-inflammatory drugs (NSAIDs) or non-NSAID analgesics
Wrist sprains involve injury to the supporting ligaments of the radiocarpal joint. Wrist sprains are rare in children but may occur in adolescent athletes who experience twisting injuries.
Mechanism of Injury
Scapholunate ligament sprains - result from excessive wrist extension with pronation (eg, a fall on an extended wrist). This is the most common of the wrist sprains.
Lunotriquetral sprains - result from sudden axial loading with wrist extension and radial deviation, causing pain along the ulnar aspect of the wrist.
Ulnar collateral ligament sprains - occur during forced hyperextension and abduction, also known as gamekeeper's thumb or skier's thumb.
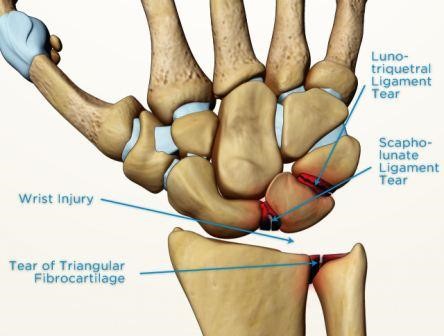
Image Source: https://www.sportsmd.com/sports-injuries/wrist-hand-injuries/scapholunate-ligament-tear/
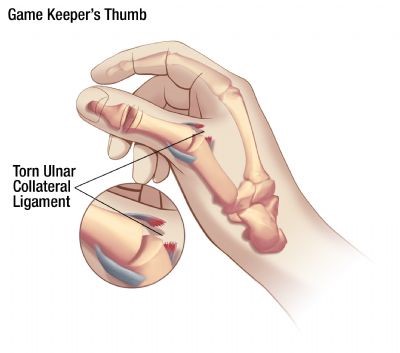
Image Source: https://www.aliem.com/2013/07/ulnar-collateral-ligament-injury/
Physical Examination
Physical exam should start with an inspection in the areas for tenderness, swelling and ecchymosis, assessment for effusion, evaluation of range of motion and neurovascular status, and comparison of the injured with the uninjured side.
Evaluation: Imaging
X-ray findings may be normal or show an increased scapholunate distance. X-ray findings are usually normal in lunotriquetral sprains.
Management
The primary goals of sprain management are to reduce swelling and inflammation.
a. Immobilization
b. Supportive Care
c. Referral to a hand specialist should be considered because untreated ligamentous injuries to the wrist may result in chronic pain and functional compromise. Orthopedic referral is recommended for scapholunate ligament injury.
Upper Extremity Injuries
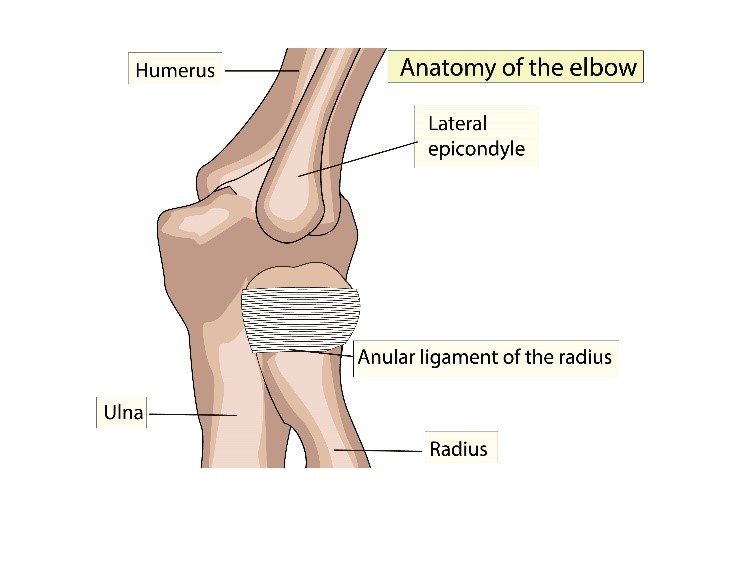
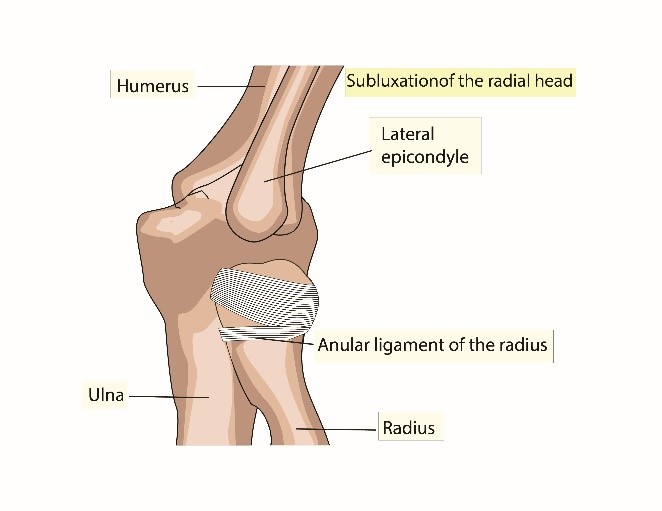
This injury is most commonly seen in children 3-5 years of age and rarely occurs after seven years of age. The lack of ossification of the proximal radial epiphysis in children less than five years of age make it more pliable and prone to slippage of the annular ligament.
Mechanism of Injury
Injury is caused by longitudinal traction applied to pronated forearm and extended elbow (e.g. Child lifted or swung by the forearm). This results in subluxation of the radial head and interposition of the annular ligament into the radiocapitellar joint.
|
|
|
Physical Examination
Initial pain subsides rapidly but child is reluctant to use the arm, choosing to keep it close to the body with elbow slightly flexed and forearm pronated. Any attempt to supinate the arm causes pain. Pain and tenderness to palpation of the lateral aspect of the elbow (around the radial head and annular ligament).
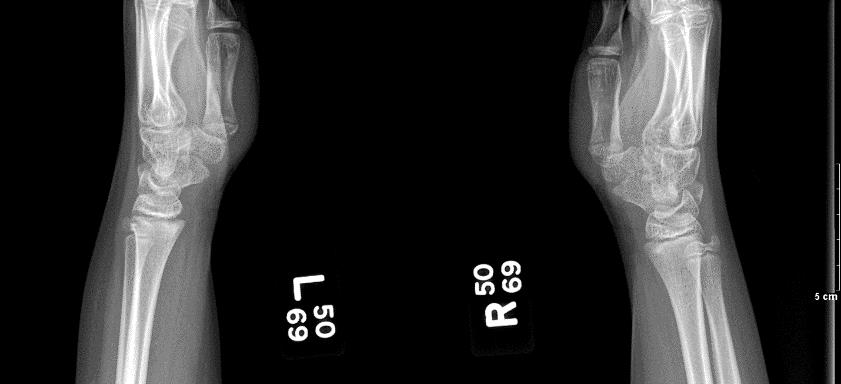
Evaluation: Imaging
X-rays are not routinely indicated with a reliable history consistent with physical exam. If X-rays are done, anteroposterior and lateral views are usually normal; many times the subluxation is reduced inadvertently when technician supinates the arm to take x-rays. If the history is inconsistent, suggestive of a possible compounding injury, or if there is noticeable significant swelling of the joint or surrounding soft tissue, obtain X-rays prior to attempting reduction.
Management
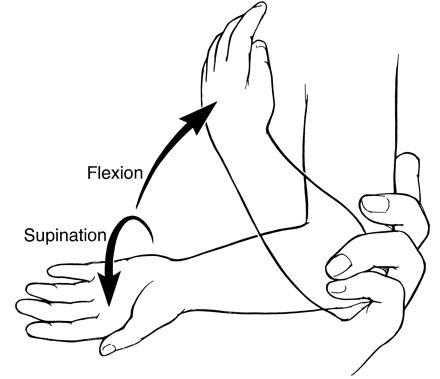
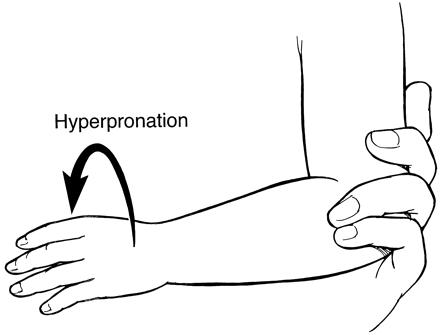
Two techniques for closed reduction (see image below). An audible or palpable click is associated with high probability of successful reduction. Child is able to use arm normally thereafter. If a definite snap or pop is not felt or if the patient fails to use the extremity, obtain x-rays if not yet done, and re-examine the entire extremity again carefully.
 |
|
|
Supination-Flexion Technique Place thumb over radial head and apply pressure. Manually supinate the arm and flex maximally - ideally past 90 degrees of flexion. |
Forced Pronation Technique Hold arm flexed 90 degrees at the elbow and hyperpronate at the wrist.
|
This condition is seen mostly in adolescent pitchers or tennis players. Typically, patients present with pain when throwing but may also present with decreased velocity and control.
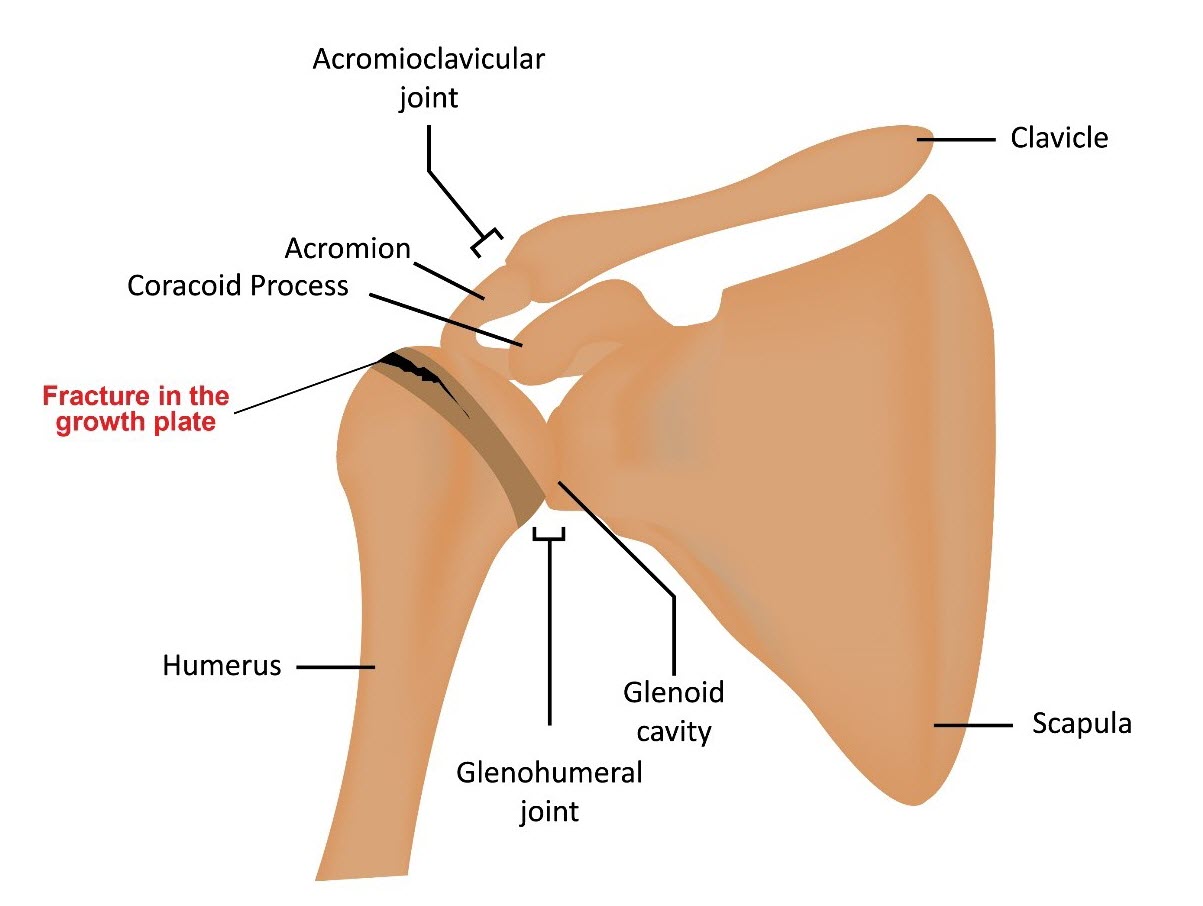
Mechanism of Injury
Overuse injury is caused by overhand pitching without proper rest, pitching/throwing without proper technique, or lack of muscle strength of the shoulder and upper back. Microtrauma at the physis (Salter Harris Type 1) of the proximal humerus can also occur. There is widening of the growth plate that result in pain and swelling at the shoulder joint.
Physical Examination
Point tenderness over the shoulder physis and reproducible pain with shoulder rotation
Evaluation: Imaging

Management
|
Little League Baseball Pitch Count Regulations |
||
|---|---|---|
|
Age |
Limits Per Game |
Rest Requirements |
|
17-18 years |
105/day |
76 or more pitches -> 4 days rest 61-75 pitches -> 3 days rest 46-60 pitches -> 2 days rest 31-45 pitches -> 1 day rest 1-20 pitches -> 0 days rest |
|
15-16 years |
95/day |
|
|
13-14 years |
95/day |
66 or more pitches -> 4 days rest 51-65 pitches -> 3 days rest 36-50 pitches -> 2 days rest 21-35 pitches -> 1 day rest 1-20 pitches -> 0 days rest |
|
11-12 years |
85/day |
|
|
9-10 years |
75/day |
|
|
7-8 years |
50/day |
|
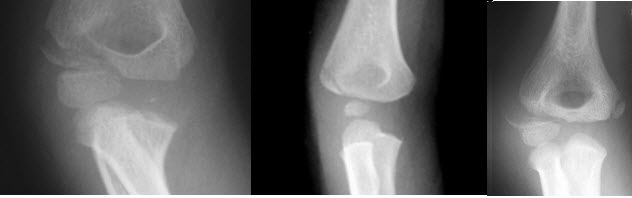
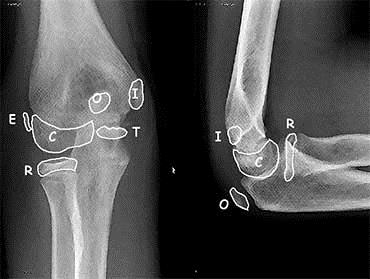
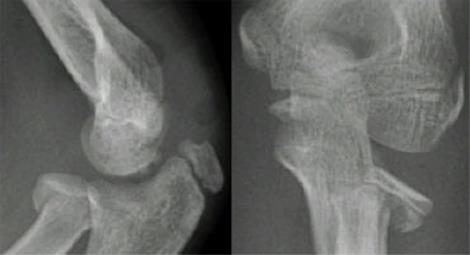
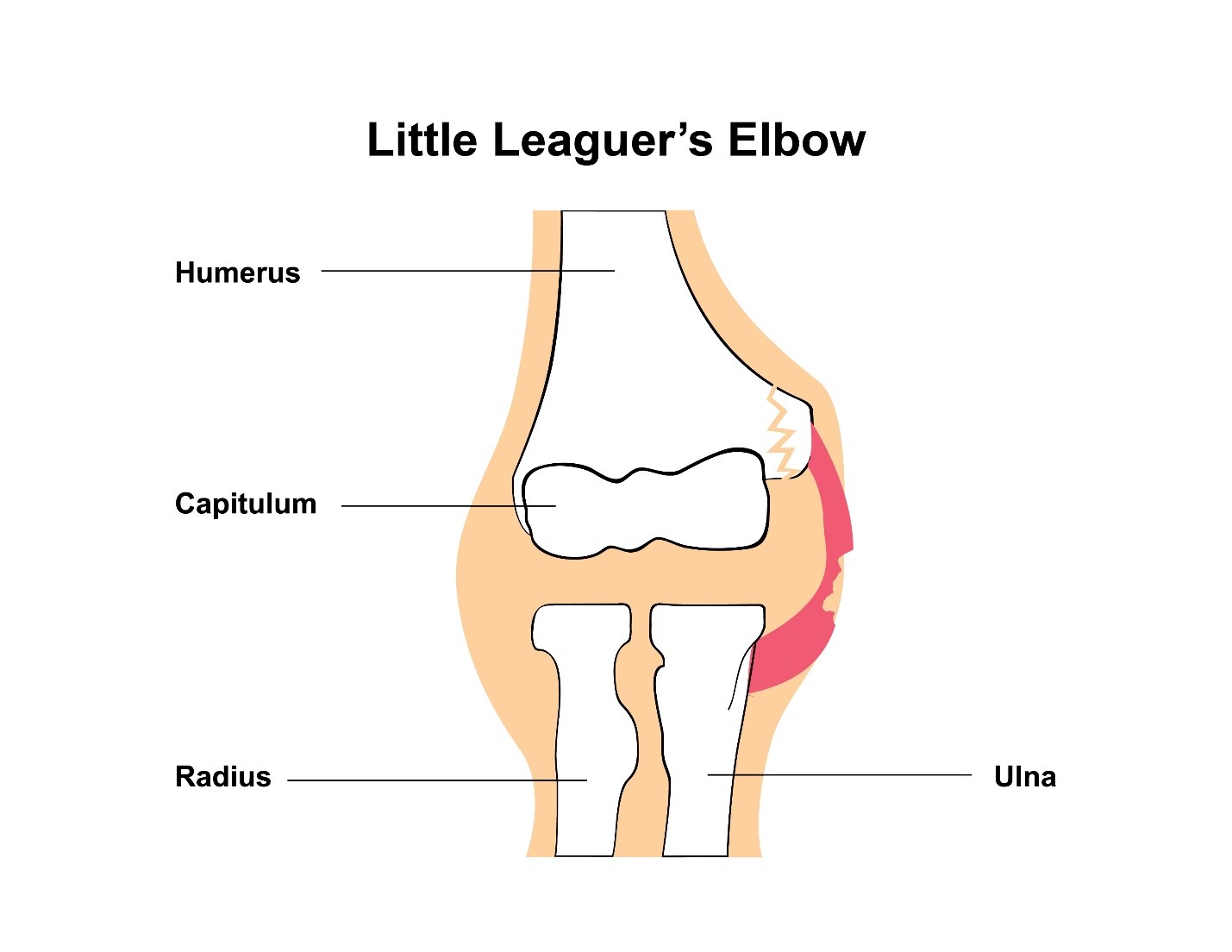
Apophysitis is defined as irritation of a bony protuberance that is a site of tendon or ligament attachment. Little leaguer's elbow is more commonly seen in active, growing children and adolescents. It is related to overuse in skeletally immature baseball pitchers (e.g. Excessive amount of pitches per game, excessive fastball speed, and continued pitching in spite of fatigue). This is a spectrum of injuries to the medial aspect of the elbow (due to excessive tension on medial epicondyle) with secondary tendinitis. The child typically develops decreased speed, accuracy and distance of pitches.
Mechanism of Injury
Injury is often associated with throwing curve balls. The excessively strong pull on the tendons and ligaments of the elbow cause repetitive microtrauma to the immature skeleton.
Physical Examination
Patient typically presents with a decrease in elbow extension. There is significant pain and swelling over the medial epicondyle accentuated by valgus stress to the elbow in extension.
Evaluation: Imaging
|
|
Management
Rest - Return to play is done only when asymptomatic
Physical Therapy - focuses on arm and forearm strengthening
Ice - to help with acute swelling and pain in the shoulder
Throwing Program - progressively increases the force and demand on the arm and shoulder until able to return to competitive play with enforcement of pitch counts
Clavicular fractures is often seen in young, active patients. It is also the most common site of all obstetrical fractures (eg. LGA infants and those requiring instruments or special maneuvers for delivery). Associated injuries may include the scapula, the ribs, the lung (pneumothorax) and even the neurovasculature.
Mechanism of Injury
Classification based on anatomic location
Group I: Middle third (most common occurring 76-85%)
Group II: Distal third (10-21%)
Group III: Medial Third (3-5%)
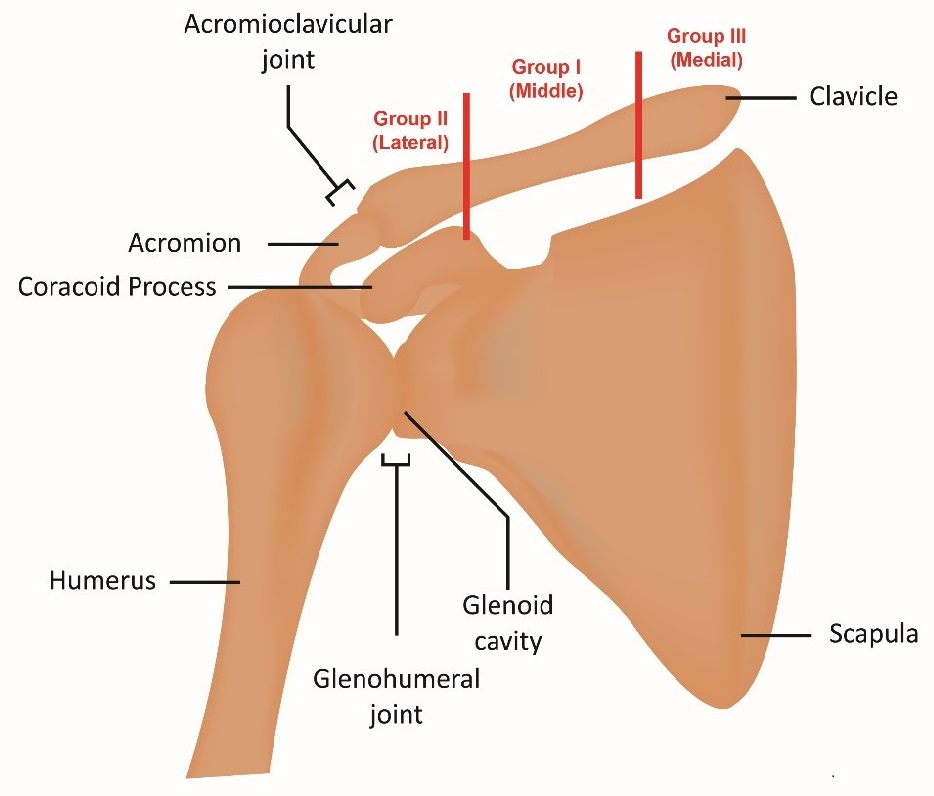
Physical Examination
Patients typically present with moderate to severe pain in the shoulder, refusal to move arm on affected side, or swelling and bruising, along with a bony deformity.
Evaluation: Imaging
Anteroposterior radiograph is the standard study used. Other views used include cephalad-caudad (helpful to assess degree of displacement), apical-oblique (suited to identify fractures in the middle 1/3), apical-lordotic and axillary lateral view. CT may be useful for medial physeal fractures and sternoclavicular injuries.
Management

ORIF method results in faster union, improved functional outcome, better cosmetic results, and improved over all shoulder recovery.
Possible complications include: hardware prominence (25-30%), neurovascular injury (3%), nonunion (1-5%), infection (4-5%), mechanical failure (1-2%) and adhesive capsulitis (4%).
|
Operative - Open Reduction, Internal Fixation (ORIF) |
||
|---|---|---|
|
ORIF method results in faster union, improved functional outcome, better cosmetic results, and improved over all shoulder recovery. |
Indication |
Relative Contraindication |
|
|
Nondisplaced fractures Skin intact Medically unfit for surgery |
Open fractures Multiple extremities injured Skin tenting or impending skin necrosis |
|
|
Comminuted fractures Fractures with 100% displacement fractures Prolonged nonunion Open fractures Floating shoulder Neurovascular involvement Significant shortening (>2 cm) Vertical fragment Infection |
Infection Severe skin condition (eg. acne) Stroke patient with little extremity usage |
| Indications for Operative and Nonoperative Management | ||
| Management
|
Indication
|
Relative Contraindication
|
|
Nonoperative
|
Nondisplaced fractures Skin intact Medically unfit for surgery
|
Open fractures Multiple extremities injured Skin tenting or impending skin necrosis
|
|
Operative
|
Comminuted fractures Fractures with 100% displacement fractures Prolonged nonunion Open fractures Floating shoulder Neurovascular involvement Significant shortening (>2 cm) Vertical fragment Infection
|
Infection Severe skin condition (eg. acne) Stroke patient with little extremity usage
|
Knee Injuries
Differential diagnoses may vary depending on the location of the knee pain.
| Anterior |
Posterior |
Lateral |
Medial |
|---|---|---|---|
|
|
|
|
(Osteochondrosis of the Knee or Tibial Tuberosity Apophysitis)
Osgood-Schlatter Disease is a common cause of chronic anterior knee pain in young athletes that presents with significant pain, tenderness and swelling at the insertion point of the patellar ligament on the tibial tubercle. The patellar ligament connects the quadriceps muscles to the superior pole of the patella and then the inferior pole of the patella to the proximal tibia at the tubercle.
Pain progressively worsens over time with continuous overuse eventually leading limitation of activity. Pain is aggravated by any direct trauma to knee, kneeling, squatting, climbing stairs or running and is relieved with rest and ice. Adolescents between the ages 9-14 who are experiencing a rapid growth phase and participating in activities or sports that involve running, jumping, cutting or squatting thereby increasing their risk for the development of OSD. Male prevalence but as female sports participation increases so has the incidence of OSD in females. Typically, unilateral knee affected (asymmetric) but bilateral in 25-50% of cases.

Note that the location of the pain distinguishes Osgood-Schlatter (pain in the tibial tuberosity) from Sinding-Larson-Johansson (pain in the inferior pole of the patella). Both conditions are due to microtrauma to the apophysis (growth plate that provides a point of attachment for the muscle and its associated tendon or ligament) in a skeletally immature but active child.
Mechanism of Injury
Exact cause is unknown but chronic repetitive trauma to the maturing proximal tibial growth plate by excessive force exerted on the secondary ossification center or apophysis by the patellar tendon leading to avulsion and tibial fragmentation with soft-tissue swelling of tubercle. The injury results in callous formation as healing occurs resulting in prominence of tubercle.
Physical Examination
Diagnosis is made by clinical exam. There is typically tenderness with soft-tissue swelling over the tibial tuberosity without erythema or warmth. Reproducible pain can be elicited with knee extension against applied resistance, during squatting with knee in fully-flexed, or with significant stress applied to quadriceps. Straight-leg raising usually is painless. Pain that is more prominent in the patellar tendon than the bony prominence is suggestive of patellar tendinopathy (jumper's knee).
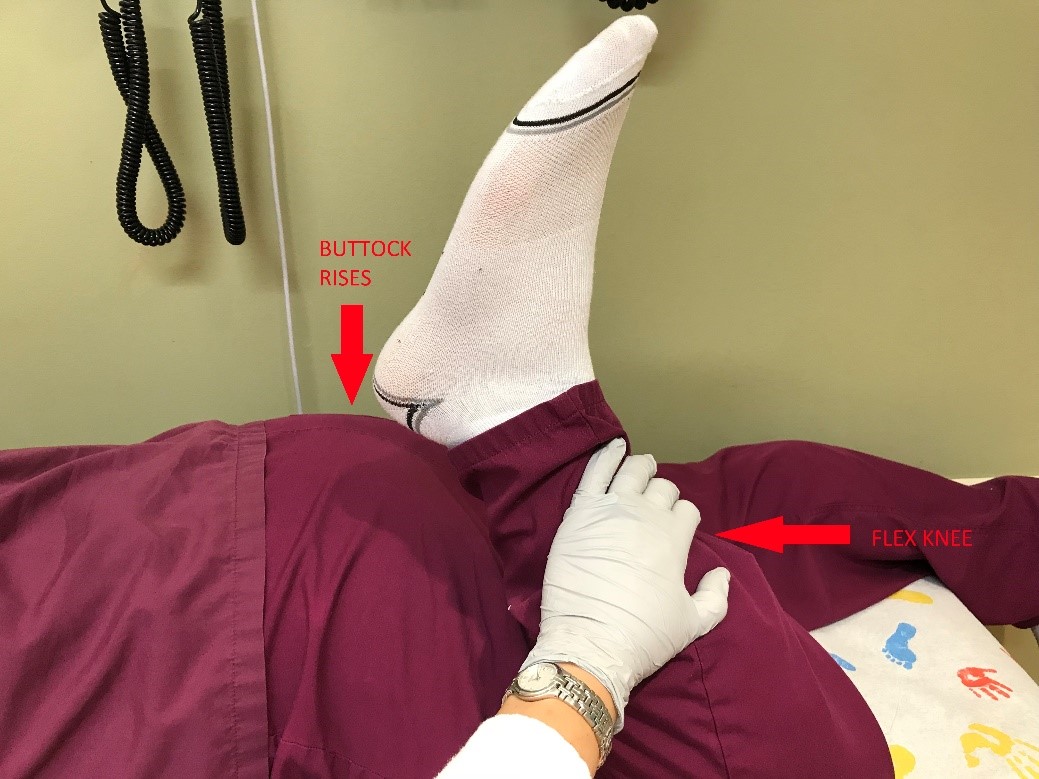
Ely Test
This test detects contracture of the rectus femoris component of the quadriceps muscle. With the patient prone, the examiner gently flexes the knee to 130 degrees. Contracture of the rectus femoris is indicated by simultaneous flexion of the hip, which causes the buttocks to rise off the table. Tight quadriceps or hamstrings have decreased elasticity or flexibility resulting in increased force on the patellar ligament.
Evaluation: Imaging
Lateral view may show soft-tissue swelling anterior to tibial tubercle. Other radiograph findings may include elevation or increased density of the tubercle, thickening or calcification of patellar ligament, or presence of bony fragment present within the patellar ligament, infrapatellar bursa edema.

Image source: http://www.radpod.org/2008/03/25/osgood-schlatter-disease/
Management
Osgood-Schlatter Disease is usually a benign and self-limiting disorder that resolves with closure of proximal tibial growth plate at 14-18 years. Tubercle prominence may be persist after growth plate closure, but pain and tenderness are no longer present.
Non-operative treatment involves "RICE" treatment for swelling reduction and analgesic medications for pain control. Limitation of activities that exacerbate symptoms is encouraged if pain does not resolve in 24 hours or pain is not tolerated. Using a brace or padding over the knee for protection and support of knee during activities (patellar tendon strap or taping between kneecap and tibial turbercle). Strengthening and stretching exercises or physical therapy can help increase flexibility of quadriceps and hamstrings. Patients with persistent pain greater than 3 months may benefit from injection of hyperosmolar dextrose (12.5%) mixed with lidocaine by the orthopedist.
Surgical intervention involves tibial tuberosity excision or ossicle resection in patients who fail conservative management. Surgery is usually not performed until the growth plates close.
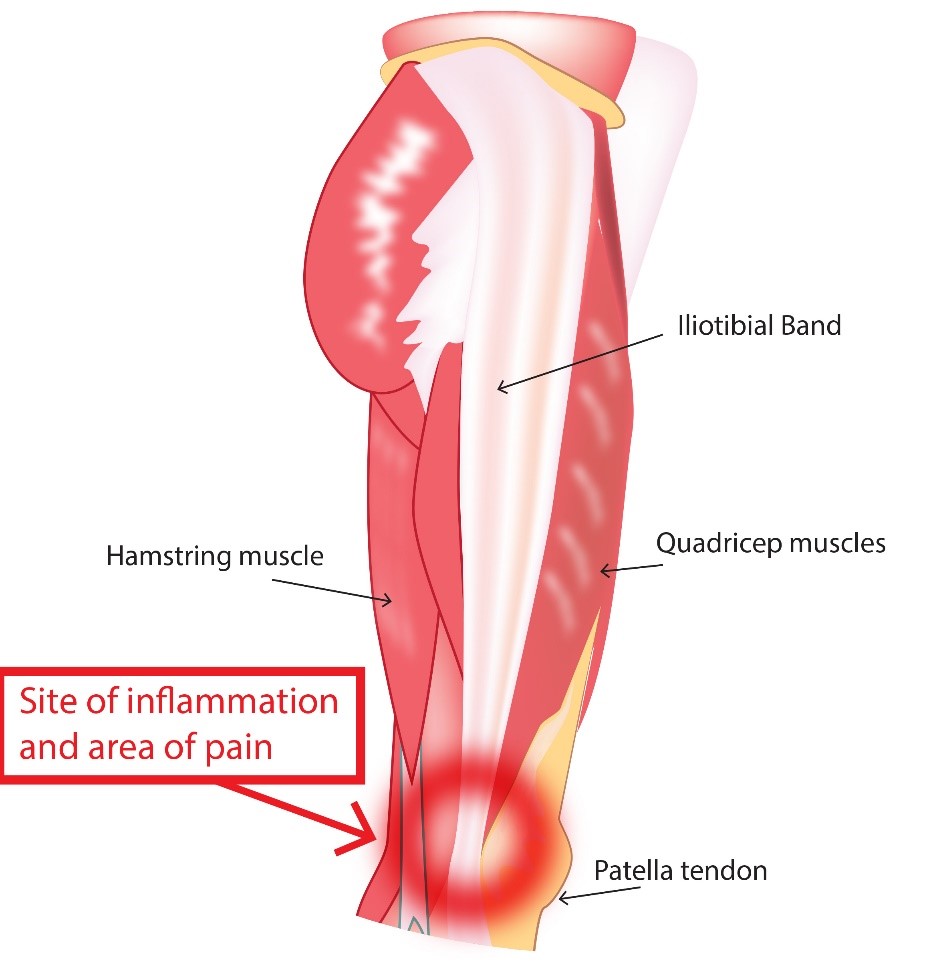
This is an overuse injury in jumping athletes. Upon presentation, they have pain localized to the superior border of the patella that worsens with activity. There is frequently associated swelling to the affected area also. Risk factors are sports that highly involve jumping (basketball, volleyball, long/high jump).
Mechanism of Injury
The injury occurs as a result of repetitive eccentric contractions ( motion of an active muscle while it is lengthening under load ) of the extensor mechanism. Microtears of the tendon most commonly at the bone-tendon interface then inflammation of the suprapatellar tendon of the quadriceps muscle.
Physical Examination
There is tenderness to deep palpation at quadriceps tendon insertion at the patella. A palpable gap over the affected area would suggest a quadriceps tendon tear. Upon evaluation the range of motion, there is pain upon knee extension but patient is able to actively extend the knee against gravity.
Evaluation: Imaging
Management
Usually a non-operative approach is the mainstay of therapy: activity modification (rest until pain is improved), NSAIDs, and physical therapy. Cortisone injections are contraindicated due to risk of tendon rupture.
The prepatellar bursa is a potential space that functions to enhance gliding of tissue over the patella. This injury is caused by excessive kneeling. It is generally seen in wrestlers. Aseptic bursitis occurs more commonly, but septic bursitis can also occur.
Physical Examination
Localized tenderness and swelling is notable over the prepatellar region (anterior to the patella or patellar tendon) but it can also be warm to touch (especially if septic).
Evaluation: Imaging
X-rays (AP and lateral views) of the knee should be obtained in all patients with suspected acute bursitis. Knee ultrasound or MRI are usually not necessary for diagnosis. In chronic bursitis, CT, MRI, or bone scintigraphy may be helpful to determine if underlying osteomyelitis is present.
Bursal aspiration by the orthopedist is the key component of evaluation of knee bursitis to exclude septic bursitis.
Management
Iliotibial Band Tendinopathy is a result of excessive friction between the iliotibial band (ITB) and lateral femoral condyle, subsequently causing ITB tensioning and inflammation. This injury is most commonly seen in runners, cyclists, and other athletes with repetitive knee flexion and extension.
 Symptoms
Symptoms
There is a localized pain over the lateral femoral condyle that is exacerbated with running. The pain is usually relieved with rest.
Physical Examination
Palpation over the lateral femoral condyle provokes localized pain. Range of motion of the affected leg elicits knee joint crepitus, reduced hip and/or knee range of motion due to pain, weakness upon hip abduction, and pain reproduced with single leg squat.
Ober test assesses the tightness of ITB. It is performed with the patient lying on the unaffected side. The examiner slightly abducts and extends the affected hip and flexes the knee. The patient is then asked to allow the affected leg to fall to the table passively, without actively adducting the hip (just letting it fall with gravity), while the examiner supports the patient's lower leg. Patients with ITB syndrome are more likely to have limited adduction of the leg with this maneuver (positive Ober test).
Image Source: https:https://www.bodyheal.com.au/blogs/sports-injuries/iliotibial-band-syndrome-symptoms-causes-treatment
Image Source: http://indianapolisfitnessandsportstraining.com/really-band-friction-syndrome-runners/

Image source: https://www.flickr.com/photos/sportex/8076561890
Evaluation: Imaging
Management
Overview
The lateral and medial menisci are thickened cartilage that act as cushions between the tibial-femoral joint. Meniscal tears occur mostly in adolescents engaged in sports including soccer, basketball, and football that involve deceleration and a sudden change in direction with the knee partially flexed and the foot planted. The medial meniscus is more commonly injured than the lateral meniscus with injury occurring through a twisting or pivoting mechanism also involving compression with or without varus/valgus applied forces.
The meniscus in the adolescent is comprised of three parts or thirds:
Tears are classified as longitudinal or radial based on the meniscal surface and as complete or incomplete according to the depth of the tear.
A meniscal tear may present initially with pain followed by swelling over a 24 hours period and/or pain aggravated by pivoting motions of the knee. A "tearing" or "popping" sensation may also be felt at the time of injury. Mechanical symptoms such as "catching" or "locking" coupled with a feeling of instability or the knee "giving out" may also be reported. The sensation of "locking" or "catching" is created by a portion of the torn meniscus interfering with the ability to fully extend the knee as the fragment interposes between the articular surfaces of the femur and tibia. Altered proprioception caused by the detached meniscal fragment moving around between the articular surfaces also results in perception of instability
Physical Examination
The type and location of the meniscal tear influence the accuracy of the physical exam with partial, horizontal, or anterior tears often resulting in a normal knee exam as these tears do not impede the normal knee mechanics. Patients with meniscal tears may present with lateral knee pain with tenderness to lateral joint line and decreased range of motion that may inhibit full extension of the knee. A joint effusion may also be present in larger or more complex meniscal tears. Effusions may reduce knee flexion and may be reported as joint stiffness.
Three tests can be used to produce the catching or locking sensation that is associated with meniscal tears.
Thessaly Test
Attempts to recreate the loading forces applied to the knee. The clinician and patient face each other while standing and hold hands for support. The patient stands on one leg with knee flexed around 20 degrees. The patient then rotates their knee and body while maintaining knee flexion which rotates the knee both internally and externally while putting force on the meniscus. Perform the test on the unaffected side first for comparison and so the patient can learn the maneuver then test the affected side. Eliciting pain or reproducing the catching/locking sensation constitutes a positive test.
McMurray Test
Involves repeated passive knee flexion and extension to assess for joint motion tenderness and to detect meniscal injury. The patient is supine with the clinician holding the patient's heel with one hand and placing the other hand along the joint line. The knee is passively flexed to as near 90 degrees as possible as the examiner rotates the tibia internally while gradually extending the knee. Repeat passive full flexion and extension of the knee with tibia in internal rotation is then followed by passive flexion of the knee with external rotation of the tibia which is repeated several times. Varus and valgus pressure are sometimes applied during passive flexion and extension to increase stress on meniscus as may help detect injury. A painful snap or click in early- or mid-extension that may be sometimes felt or heard or pain elicited along the joint line with maneuver are suggestive of meniscal tear. This maneuver tests the posterior and middle portions of the meniscus and therefore anterior or anterolateral tears may not be detected reliably with this test. Thus, a negative test does not completely rule-out a meniscal tear.
Apley Compression Test
The patient in prone position with affected knee flexed 90 degrees while the examiner their own hand or knee to stabilize the patient's thigh. The clinician then moves the patient's heel toward the floor or exam table while rotating the foot internally and externally and the knee is extended. This maneuver results in the compression of the meniscus between the tibial plateau and the femoral condyles. Eliciting pain with compression of meniscus results in a positive test.
Evaluation: Imaging
Evaluation: Other
Management
Management depends on the type of tear and on the presence of instability, mechanical symptoms, persistent effusion or hemarthrosis. Small tears that are rarely symptomatic and do not interfere with normal knee mechanics and function can be managed conservatively.
Conservative measures: Rest the knee. Avoid maneuvers or activities that apply pressure on the knee joint until swelling subsides including squatting, kneeling, pivoting, or movements that require repetitive flexion/extension of knee joint like climbing stairs. Apply ice to the knee for 15-20 minutes every 4-6 hours with leg elevated may help reduce pain and swelling. Use crutches to reduce weight-bearing on affected knee. Utilize a knee brace that restrains patellar motion to prevent knee "giving out." Pain management, as needed. Conservative management is likely to be successful in cases where symptoms develop more slowly over 24-48 hours (rather than immediately), minimal swelling is present, full range of motion of the knee with pain is present only during full flexion or nearly full flexion of knee, or McMurray Test elicits pain only during deep flexion.
Physical therapy
Orthopedic referral should be made for determining type of tear and degree of tear and whether surgical intervention is necessary. Immediate orthopedic referral should be made for large complex tears with persistent effusion, tears resulting in frequent mechanical symptoms, or "locking" of knee with extension as surgical intervention is likely necessary.
Arthroscopic or open knee surgery with partial meniscectomy is preferred over total meniscectomy as it results in less recovery time and it reduces risk of developing of osteoarthritis. Osteochondritis dissecans of the lateral femoral condyle is a rare complication following partial and total meniscectomy secondary to repetitive compression of the immature chondral structures.
Surgical Intervention is likely to be required when the following factors are present:
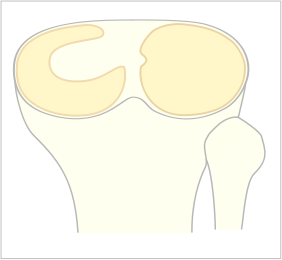
Overview
Discoid Meniscus is a term that describes an anatomic abnormality of the shape of the meniscus that results in a larger, thicker meniscus that resembles a "disc" rather than the normal "crescent" shape. It typically involves the lateral meniscus but can be bilateral in a small percentage of affected individuals.
A specific cause for developing a discoid meniscus is unknown but may be a congenital anomaly or due to other contributing genetic and familial factors. Discoid menisci demonstrate a "disorganized collagen fiber scaffold" formation which increases the incidence of meniscal tears with horizontal tears being the most common.
Patients with this abnormally-shaped meniscus may be asymptomatic especially in early childhood as the menisci are stable and no tearing has occurred. Older children and adolescents may present with chronic pain, an intermittent history of knee popping or clicking, effusion, quadriceps atrophy, limited ROM, as well as other mechanical symptoms such as locking or "giving way".
Classification of discoid menisci is based meniscus shape and its stability based on the degree of hypermobility and peripheral rim detachment. Unstable incomplete or complete menisci can be further differentiated by location of instability (anterior, middle or posterior horn).
Image source from Wikimedia Commons: https://commons.wikimedia.org/wiki/File:Scheibenmeniscus.svg
Physical Examination
Tenderness along the joint line, effusion, and meniscus may be felt when laterally snapping out of joint. An unstable discoid meniscus secondary to peripheral rim detachment may result in the meniscus moving into the intercondylar fossa when the knee is extended resulting in a snapping sensation, audible crepitus, and a swelling or bulge noted to the anterior joint line. A "clunk" also may be felt or heard at end of flexion. The McMurray Test as discussed above may be used to detect a discoid meniscal tear.
Evaluation: Imaging

Source: images.radiopaedia.org
Management
Asymptomatic discoid menisci do not require treatment even when snapping is present. However, management includes observation if found incidentally during another study as discoid menisci are vulnerable to tears.
Discoid menisci that are symptomatic generally require surgical intervention with partial meniscectomy being more common than total meniscectomy to reduce risk of osteoarthritis that often results when the entire meniscus is removed. Arthroscopic partial meniscectomy or "saucerization" involves the removal of central portion of meniscus with preservation of the stable peripheral rim with or without repair of peripheral rim detachments. This procedure effectively reshapes from disc into crescent-shape which is more anatomically correct but the remaining portion of the discoid meniscus is still prone to tears.
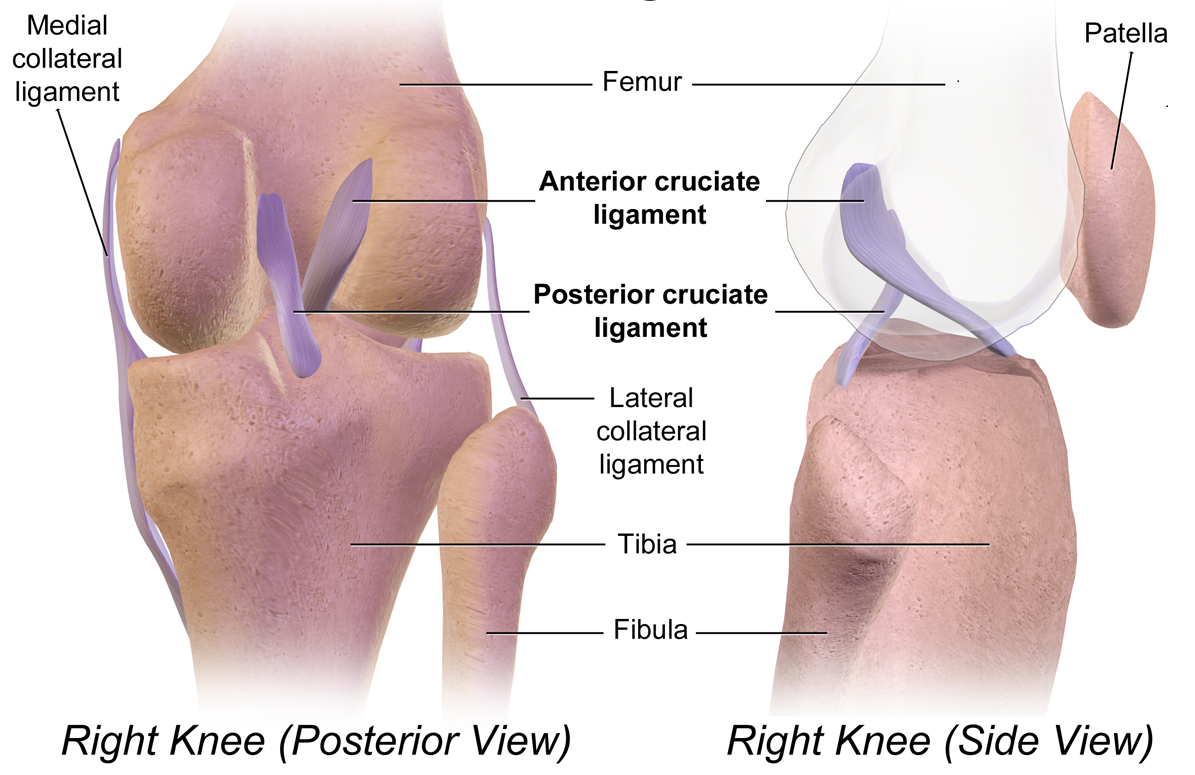
Image Source from Wikimedia Commons: https://commons.wikimedia.org/wiki/File:Cruciate_Ligaments.png
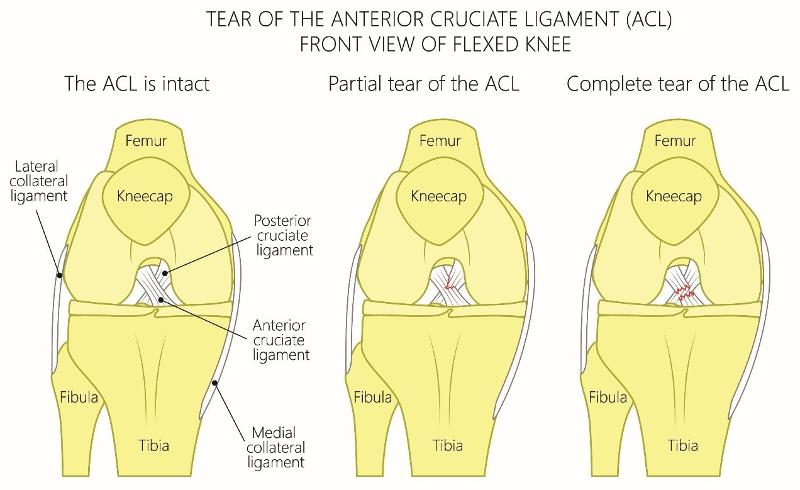
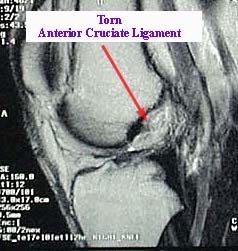
ACL tears are a common injury in adolescents participating in sports that involves running and cutting such as volleyball, soccer, basketball, skiing and football. Most common mechanism typically involves a low-energy noncontact injury that involves sudden deceleration or sudden stop combined with a twisting or pivoting motion that increased valgus stress or lateral bending of the knee.
A non-contact injury can occur when running and then suddenly changing direction in effect twisting the knee or via contact injury when the foot is planted on ground and a subsequent valgus force is applied to the knee during a collision (common in football); or the athlete falls in a way that results in rotation or lateral bending of the knee. ACL injury can also be secondary to high-impact force such as in a motor vehicle collision with direct force applied to the lateral knee.
Female athletes are more likely than males to sustain ACL injury due to differences in muscle strength and development, poor biomechanics, and the effects of estrogen on ligament laxity, strength, and flexibility.
Patients typically present with lateral knee pain, effusion, decreased ROM, and inability to bear weight immediately after injury. Patients may report a "popping" sensation at time of injury. Pain and swelling gradually subside over after several weeks as does the ability to bear weight. However patients often report instability of the knee with episodes of knee "giving out" or "giving away" when performing pivoting or cutting motions.
Physical Examination
ACL on physical exam usually involves the Anterior Drawer, Lachman, and Pivot Shift tests which can detect increased forward motion of the affected knee albeit these test have less sensitivity if performed immediately after injury due to presence of pain and swelling.
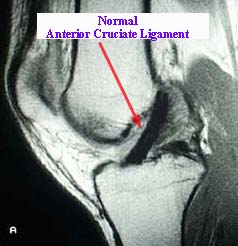
Evaluation: Imaging
Diagnosis can be made with physical exam findings but imaging can support clinical diagnosis.

|
|
|
Source: emedx.com
Management
In the acute setting, patients with history and findings suggestive of ACL injury should be placed in a knee brace and given crutches to avoid weight-bearing protecting against further injury. Elective outpatient referral to orthopedic surgeon should be placed with evaluation made within 7-14 days post-injury.
Non-operative treatment is an option for those that do not plan to return to sports activities and includes physical therapy with quadriceps strengthening and neuromuscular rehabilitation.
Surgical reconstruction is usually required for those desiring to return to sports activities as recurrent knee instability may interfere with ability to play sports that involve pivoting motion.
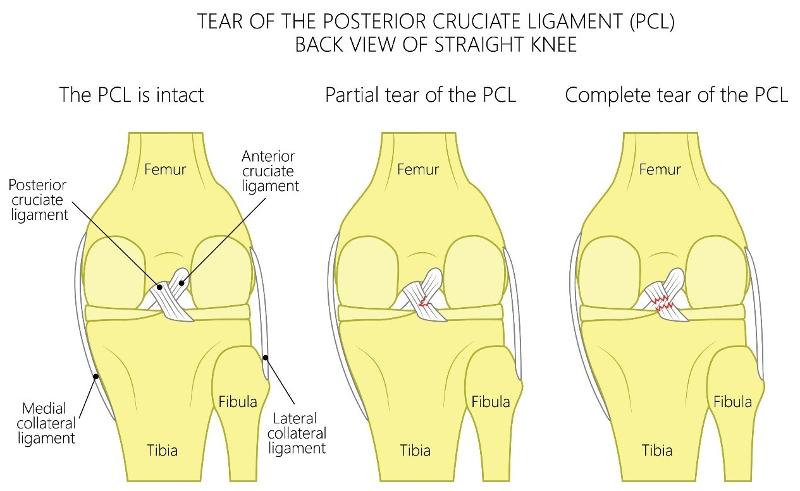
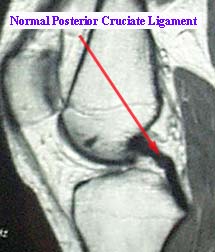
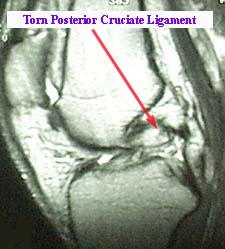
PCL injuries are less common than ACL injuries in athletic activities with injury occurring secondary to a fall with knee in flexion and foot in plantarflexion or due to a direct blow or posterior sheer force applied to the anterior knee. The PCL and the posterior capsule may also be injured with hyperextension or hyperflexion of the knee with or without a direct posterior force. PCL injury can also occur in motor vehicle accidents when a posteriorly directed force is applied to a knee in a fixed position and often due to a dashboard hitting the flexed knee.
Patient may present with knee instability especially if the injury also involves other posterolateral knee structures. However, isolated PCL injuries albeit rare may be more difficult to detect when other structures not involved. A "pop" may not have been felt at time of injury as opposed to ACL injury. Patient may have mild-to-moderate effusion and a limp noted during ambulation suggesting pain with weight-bearing. Patients may also report posterior knee pain especially when kneeling down or squatting and may demonstrate loss of terminal knee flexion and unable to bend knee the last 10-20 degrees. Patient may describe generalized knee pain or that something is wrong with their knee but unable to be more specific.
Isolated PCL injuries can be classified as acute or chronic. Acute injuries often present with antalgic gait as well as other gait abnormal gait patterns depending on extent of injury and patient's specific anatomy.
Physical Examination
Grades of PCL injury are based on Posterior Drawer Test:
Grade 1 (0-5 mm posterior displacement) – anterior border of medial tibial plateau can be posteriorly displaced but still remains anterior in relation to medial femoral condyle; few fibers are torn.
Grade 2 (6-10 mm posterior displacement) – anterior border of medial tibial plateau can be posteriorly displaced but is even with the medial femoral condyle.
Grade 3 (>10 mm posterior displacement) – anterior border of medial tibial plateau can be posteriorly displaced past the medial femoral condyle.
Evaluation: Imaging
Diagnosis can be made with physical exam findings but imaging can support clinical diagnosis.
|
|
|
Image source: emedx.com
Management
In acute setting, patients with history and findings suggestive of ACL injury should be placed in a knee brace and given crutches to reduce weight-bearing and to protect against further injury.
Elective outpatient referral to orthopedic surgeon should be placed with evaluation made within 7-14 days post-injury.
Non-operative treatment is an option for those that do not plan to return to sports activities and includes physical therapy with quadriceps strengthening and neuromuscular rehabilitation. For those desiring to return to sports activities, surgical reconstruction is usually required.
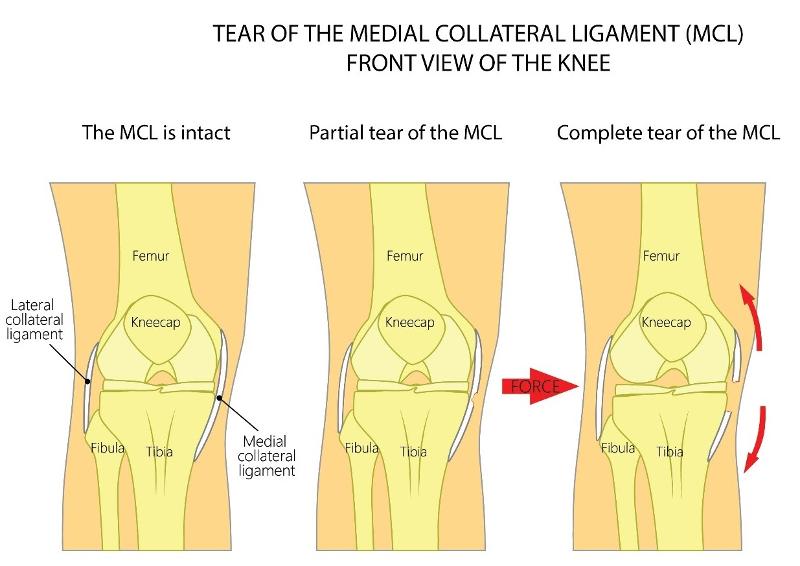
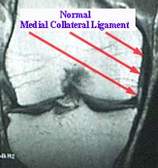
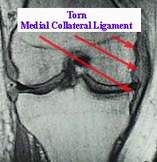
MCL tears occur when a valgus stress is applied to the lateral side of the knee suddenly forcing the knee medially into a "knocked knee" position. MCL injuries are more likely to involve other knee structures and associated meniscal tears.
Patients typically present with medial knee pain following a direct contact or collision with a valgus force applied to lateral knee while the foot is planted. Noncontact MCL injury may occur due to an abrupt valgus movement the results in the "knocked knee" deformation or knee bending medially while the knee is hyperextended with some external tibial rotation. Often occurs when an athlete catches their shoe, cleat, ski, or skate on a surface as they are quickly changing direction. Patients frequently report a sensation of knee instability especially during standing or walking. Swelling and mechanical symptoms such as locking and the knee "giving out" may also be present.
Physical Examination
The most common finding on exam is medial knee tenderness and localized soft tissue swelling. Valgus stress may reveal a widening of the knee joint.
Grades of MCL Tears
|
Grade 1 (0-5 mm of medial knee opening) - Mild tear or sprain of the ligament with some localized tenderness but no laxity or mechanical symptoms as only a few fibers are involved. Grade 2 (6-10 mm of medial knee opening) - Partial or moderate tear of the ligament with presence of localized or diffuse tenderness along the lateral or posterolateral knee. Some swelling and mild-to-moderate laxity are present but a solid endpoint is preserved indicating some ligamentous integrity is still intact. Grade 3 (> 10 mm of medial knee opening) - Complete tear of ligament with variable amount of pain. Laxity without a solid endpoint that results in mechanical symptoms and frequently associated with injury of other ligaments. |
Abduction Stress Test (also known as Valgus Stress Testing)
This is the most appropriate test for determining the extent of MCL injury. The clinician positions themselves such that one hand is placed on the lateral side of the knee to stabilize femur and the other hand is placed around the medial ankle. The clinician then pushes the knee medially while pulling the ankle laterally which opens the knee joint on the medial side. This maneuver is performed with the knee at both full extension and 30 degrees of flexion. Pain or a gap noted to the medial joint line at approximately 30 degrees indicates of ligamentous laxity and a partial tear of the MCL. Laxity at 0 degrees of flexion suggests possible injury to ACL, PCL, posteriomedial corner, and/or posterior oblique ligament.
Evaluation: Imaging
Minor injury of the MCL does not require imaging as damage is not usually seen on plain radiographs.
|
|
|
Image source: emedx.com
Management
Initial management of MCL injury is conservative management with rest, ice, immobilization and pain management as discussed in more detail under meniscal injuries. LCL injuries are managed similarly to MCL injury (see above)
Management is determined by grade of injury
Grade 1 - Crutches for up to 1 weeks and a hinged-brace worn for 4-5 weeks for all weight-bearing as it stabilizes medial and lateral knee but allows for flexion and extension of knee.
Grade 2 - Crutches and knee immobilizer for 1-3 weeks to reduce pain followed by gradual partial weight-bearing starting in week 2 or 3. Hinged-brace can be employed once partial weight bearing is achieved.
Grade 3 - Crutches and immobilization and non-weight bearing. Orthopedic referral as surgical intervention is usually required and performed two weeks post-injury.
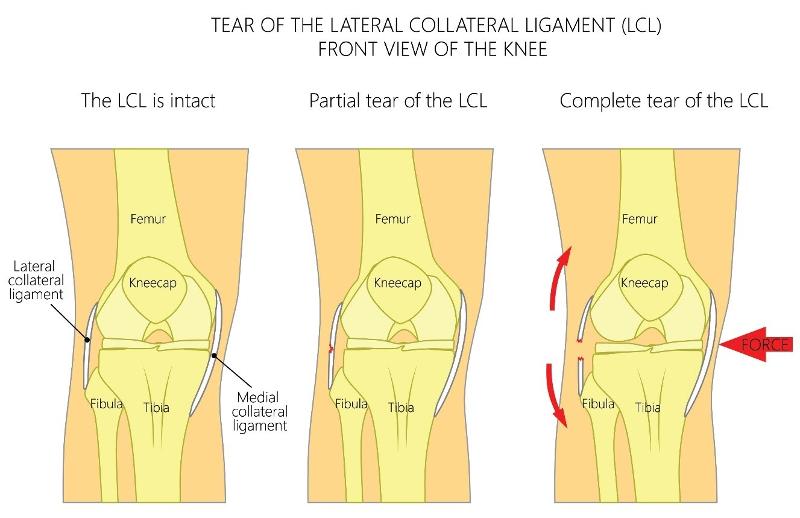
Isolated LCL injuries are the second least common knee injuries with isolated PCL tears being the least common. Isolated LCL tears occur when a varus stress is applied to the inside or medial side of the knee forcing the knee laterally LCL injuries are more likely to occur secondary to a high-energy impact injury that involves multiple knee structures such as the posterolateral corner of the knee, the lateral meniscus, the posterior cruciate ligament (PCL) and/or the anterior cruciate ligament.
Patients typically present with lateral or posterolateral knee pain after sustaining a direct hit or contact to the medial or anteromedial portion of the knee while the knee is fully extended. This often occurs in football when a player is being tackled and a posterior varus force is applied to medial knee while the foot is planted and the knee hyperextended.
Noncontact LCL injury may occur due to an abrupt varus movement results in the knee bending laterally while the knee is hyperextended. Therefore, a varus stress combined with some degree of hyperextension and/or external tibial rotation results in LCL injury.
Patients frequently report a sensation of knee instability especially during standing or walking. Swelling and mechanical symptoms such as locking and the knee giving out may also be present.
Physical Examination
Evaluation: Imaging
Management
Management of LCL tears is similar to MCL tears (see above).
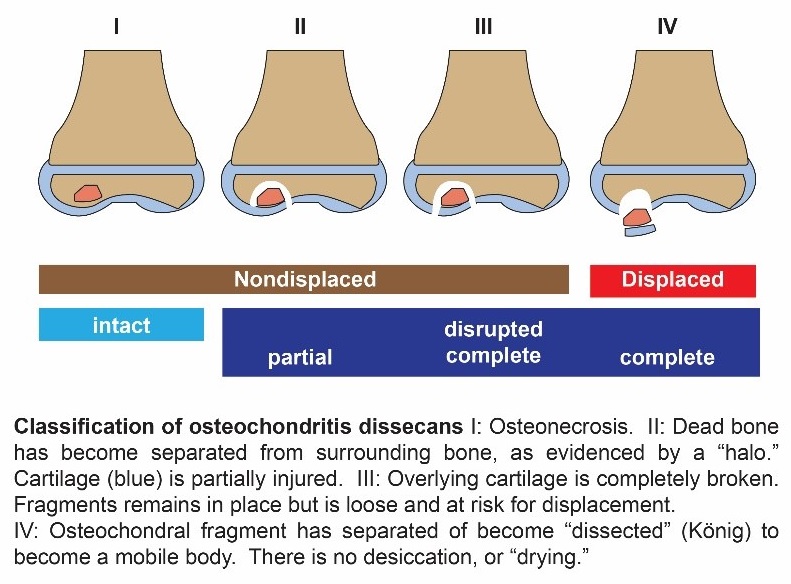
Osteochondritis Dissecans is called Juvenile OCD in skeletally immature patients or patients with open growth plates or physes.
OCD involves a lesion where a localized portion of subchondral bone and its corresponding articular cartilage become detached from the underlying bone resulting in ischemia and bone death. OCD may occur in knee, ankle, or elbow.
The ischemic bone fragment is considered stable if it remains in its original position but is classified as unstable if the fragment becomes displaced and is moving freely around the joint. Occurs most often in rapidly growing active school-aged children and adolescents. Males are more likely than females to develop OCD by a ratio of 2:1. Most common region for an OCD lesion is the lateral part of the medial femoral condyle (bilateral in 25% of cases).
Patient presents with knee pain and swelling with mechanical symptoms that can include catching or locking, sensation of knee instability or knee "giving out" as a displaced bone fragment interferes with normal range of motion
Mechanism of Injury
OCD involves a combination of traumatic injury to the knee with resulting ischemia and necrosis (death) of a segment of subchondral bone and its adjacent trabecular or spongy bone. The overlying articular cartilage attached to this area of necrotic bone remains viable as it receives it blood supply and nutrients from the synovial fluid. The necrotic portion of bone is gradually reabsorbed and is progressively replaced by new viable bone. A new trauma to the same area can result in disruption of the cartilage with dislodgment of the bone fragment leading to a loose or unattached body floating within the knee joint.
Physical Examination
Patients usually complain of non-specific, progressively worsening knee pain aggravated by activity or exercise. Development of intermittent swelling, crepitus, and joint stiffness during and after activity typically occur. Often, there is a sensation a mobile body or fragment in the joint interfering with mechanical function with catching or locking of knee or a feeling of instability with knee "giving out" and may develop an antalgic gait with lateral rotation of the foot on affected side to reduce pain with weight-bearing. Full range of motion is usually retained but tenderness when direct pressure is applied over the medial femoral condyle with the knee in full-flexion is indicative of OCD.
Wilson Sign: test used to diagnose OCD lesions of the lateral portion of the medial femoral condyle. The patient sits with the knee flexed over the exam table. The examiner actively extends the knee while medially rotating the tibia which elicits increasing pain as extension continues (or when knee reaches about 30 degrees of flexion). The maneuver is halted at this point and when the tibia is laterally rotated and the pain completely subsides.
Evaluation: Imaging
OCD lesions can be classified based on imaging findings (plain radiograph, MRI, or arthroscopy).
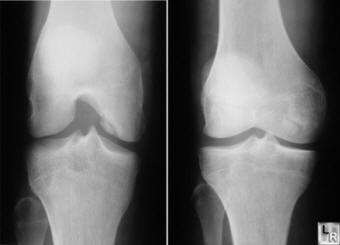

Image source: learning radiology.com
Management
Treatment is determined by OCD severity or classification according to Berndt and Hardy:
Stage I – Small compressed, non-displaced bone fragment
Stage II – Partially detached bone fragment
Stage III – Completely detached, non-displaced bone fragment
Stage IV – Completely detached, displaced bone fragment
Non-Surgical Interventions. Conservative management is usually adequate for stage I - III OCD lesions. Non-displaced fragments can be treated non-operatively through conservative measures that include NSAIDs/analgesics and no sports participation with resumption of activities only after symptoms completely resolve or imaging demonstrates complete healing of lesion. Immobilization with casting or hinged braces with limited weight-bearing for 6-12 weeks dependent on duration of healing. Physical Therapy for strengthening and increasing joint mobility after evidence of healing and weight-bearing with ambulation; swimming and cycling are often used for rehabilitation as these activities as they build muscle strength with low impact on joint.
Surgical Intervention. Indications for surgical intervention include:
Stage IV lesions which indicates a detached and displaced bony fragment
Lesion that have not responded to non-surgical treatment after 4-6 months
Lesions > 400 mm in size
Arthroscopy or arthrotomy can be uses to remove displaced fragments if non-weight bearing surface is not involved. Surgical replacement or reattachment of the fragment to the adjacent bed with a pin is required when the weight-bearing surface is involved.
Prognosis
OCD lesions that occur in the first decade have a better prognosis for healing compared to lesions that occur in second decade.
Patellar instability and patellar dislocation may occur from a direct blow, tight lateral structures (ilitobial band or vastus lateralis), or ligamentous laxity (Ehlers-Danlos). It presents with knee instability with anterior knee pain.
Mechanism of Injury
This is typically a noncontact twisting injury with the knee extended and foot externally rotated. Patient will usually reflexively contract quadriceps subsequently reducing the patella. Osteochondral fractures frequently occur as the patella relocates.
Direct blow is a less common mechanism. Examples include knee to knee collision in basketball, or football helmet to the side of the knee.
Physical Examination

Evaluation: Imaging
Views:
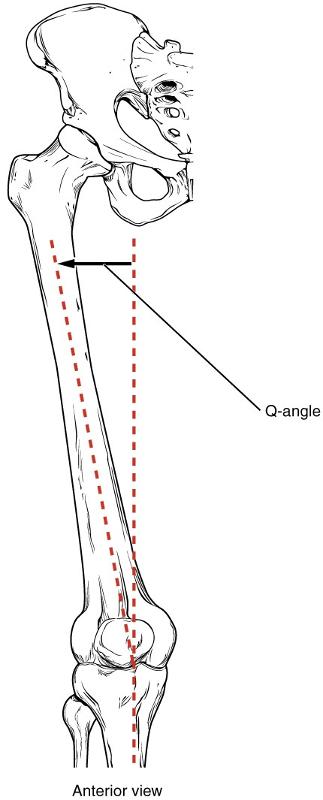
Increased Q angle: increased angle between the force vector of the quadriceps and the patellar tendon.
Management
Image source from Widimedia Commons: https://commons.wikimedia.org/wiki/File:818_Femur_Q_Angle.jpg
Muscle Injuries/Strain
Muscle strain occurs when a muscle is stretched too much, too quickly, or works too hard. Sudden or excessive forceful eccentric contraction (muscle lengthens as it contracts) of the muscle causes overstretching which results in tearing of the muscle fibers.This sometimes makes the muscle tear. Muscles that are commonly strained include those in the back, neck, and back of the leg. Symptoms of muscle strain include muscle spasms or tightness, swelling, bruising, muscle weakness, or inability to move the muscle.
Physical Examination
Evaluation: Imaging
Management
|
Supportive Care "RICEAS" |
|
Rest and avoid movements/activities that can reproduce pain Ice: Apply on the painful muscle every 1-2 hours for 15 minutes each time for up to two days. Place thin towel between the ice and skin Compression: wrap the affected muscle with an elastic bandage to help support the muscle Elevation: raise the muscle above the level of the heart Analgesic Stretch/Exercise: After pain resolves, gently stretch and exercise the muscle as it can help strengthen the muscle |
Refer to Orthopedic team for suspicions of muscle tear.
Pain Control
Over-the-Counter Medications. Non-prescribed analgesics may be used for mild pain.
Prescription Medications
These medications are prescribed for moderate to severe pain or pain refractory to non-opioid analgesics.
Acetaminophen with Codeine - schedule III controlled substance and does not require triplicate to prescribe
Tramadol - schedule IV controlled substance and does not require triplicate to prescribe. This is a weak opioid related to codeine and is less likely to be associated with respiratory depression than stronger opioids. It is not recommended for patients under 17 years of age. Tramadol can also lower seizure threshold. It should not be used in patients on antidepressants.
Oxycodone or Hydrocodone - schedule II narcotics which require triplicate to prescribe. These are stronger opioids related to codeine and contain acetaminophen.
Trade names
Vicodin (Hydrocodone/Acetaminophen)
Lortab (Hydrocodone/Acetaminophen)
Norco (Hydrocodone/Acetaminophen)
Percocet (Oxycodone/Acetaminophen)
Liquid formulations available Lortab elixir (7.5mg hydrocodone/325mg acetaminophen)
Opioids - If opioids are needed for breakthrough pain, continue for 72 hours. Re-evaluation is warranted.
Non-Accidental Musculoskeletal Injuries
In a clinical setting where musculoskeletal injury is the chief complaint, it is imperative to maintain a threshold of suspicion for physical abuse as the primary cause of an injury. Non-accidental injuries may be difficult to recognize since caretakers rarely disclose maltreatment, some children cannot provide a history, and signs and symptoms of physical abuse may be subtle or confused with other common pediatric diagnoses.
Signs & Symptoms
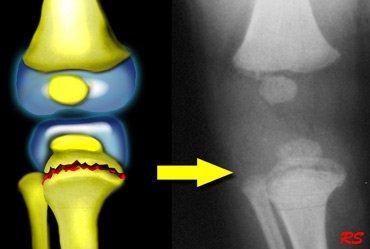
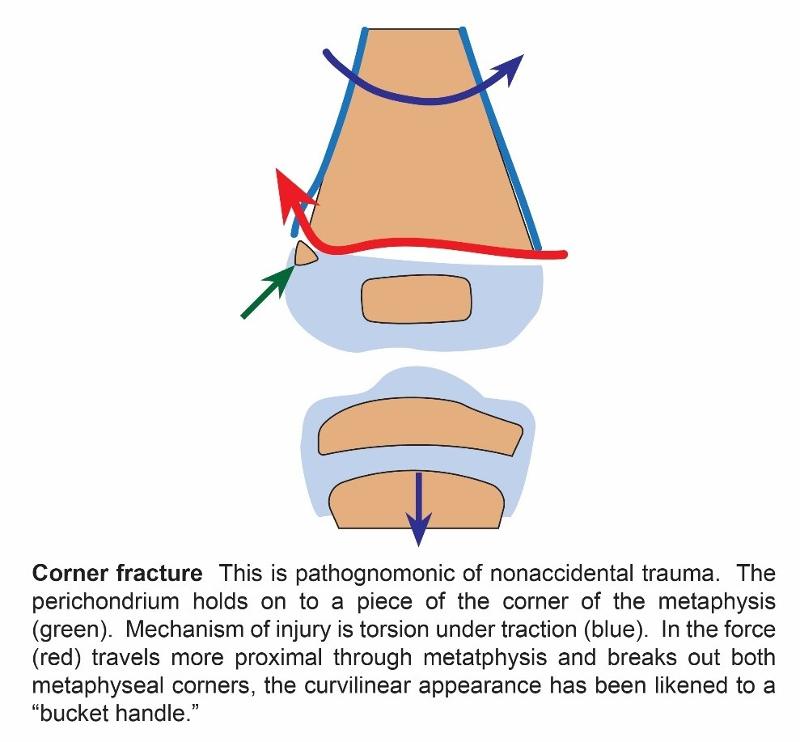
a. Corner fracture, also known as bucket handle fracture, is a metaphyseal fracture that is pathognomonic of non-accidental trauma. (see below)
|
|
|
Image source: Radiology Assistant
b. Scapula fractures
c. Spinous process
d. Sternum fractures
e. Skull fractures
f. Multiple fractures in various stages of healing
g. Bilateral fractures
h. Long bone fractures (particularly femur and humerus spiral fractures) in non-mobile infants
i. Metaphyseal fractures
j. Frequency of fractures: humerus > tibia > femur
k. Diaphyseal fractures are four times more common than metaphyseal
l. Posterioir Rib Fractures (see below)
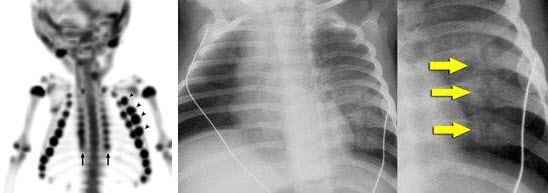
Image source: Radiology Assistant
4. Seeking medical care at different facilities for repeat events.
5. Associated risk factors for abuse include prematurity, parental youth, and unmarried status
There are medical conditions which can predispose children to have bony abnormalities making them more prone to fractures. These conditions warrant further work-up. It is important to consider these as etiology of the fracture and not exclusively from abuse.
Evaluation: Imaging
Management
Physicians are legally obligated to report suspected child abuse and neglect. Physicians are granted immunity from civil and criminal liability if they report in good faith but may be charged with a crime for failure to report.
It is important to know the law and resources specific to your state.
|
The Texas Abuse Hotline, via Texas Department of Family & Protective Services. www.txabusehotline.org 1-800-252-5400 |
References and Sources
Atanda, Alfred, Deepak Reddy, Jaime A. Rice, and Michael A. Terry. "Injuries and Chronic Conditions of the Knee in Young Athletes." Pediatrics in Review Nov 2009, 30 (11) 419-430; DOI: 10.1542/pir.30-11-419.
Beaty, James et al. Rockwood and Wilkins Fractures in Children 7th edition. PA: 2010.
Canares, Theree, Lockhart, Gregory."Sprains." Pediatrics in Review Jan 2013, 34 (1) 47-49.
Cardone, Dennis A., DO & Jacobs, Bret C., DO, MA (2016). Meniscal Injury of the knee. In T.W. Post, K. Fields & J. Grayzel (Eds.), UptoDate.
Available from https://www.uptodate.com/contents/meniscal-injury-of-the-knee?source=search_result&search=meniscal%20injury&selectedTitle=1~51
Diab, Mohammad. Practice of Paediatric Orthopaedics. New York: 2016.
Friedberg, Ryan P., MD (2016). Anterior cruciate ligament injury. In T.W. Post, K. Fields & J. Grayzel (Eds.), UptoDate. Available from https://www.uptodate.com/contents/anterior-cruciate-ligament-injury?source=search_result&search=anterior%20cruciate%20ligament%20injury&selectedTitle=1~29
Grogan, Dennis P., and John A. Ogden. "Knee and Ankle Injuries in Children."Pediatrics in Review Nov 1992, 13 (11) 429-434; DOI: 10.1542/pir.13-11-429.
Hergenroeder, Albert C., MD & Harvey, Brian S., DO (2016). Osteochondritis dissecans (OCD): Clinical manifestations and diagnosis. In T.W. Post, R. Bachur & J. Wiley (Eds.), UptoDate. Available from https://www.uptodate.com/contents/osteochondritis-dissecans-ocd-clinical-manifestations-and-diagnosis?source=search_result&search=osteochondritis%20dissecans&selectedTitle=2~26
Kienstra, Andrew J., MD & Macias, Charles G., MD, MPH (2014). Osgood-Schlatter disease (tibial tuberosity avulsion). In T.W. Post, P. Williams, J. Singer & J Wiley (Eds.), UptoDate. Available from https://www.uptodate.com/contents/osgood-schlatter-disease-tibial-tuberosity avulsion?source=search_result&search=osgood%20schlatter&selectedTitle=1~57
Kim, Jae-Gyoon, Seung-Woo Han, and Dae-Hee Lee. Diagnosis and Treatment of Discoid Meniscus. Knee Surgery & Related Research 28.4 (2016): 255-262. PMC. Web. 23 Jan. 2017.
Knee Pain and Osgood-Schlatter Disease. healthychildren.org. American Academy of Pediatrics. 20 Nov. 2015. Web. 12 Jan. 2017. Available from https://www.healthychildren.org/English/health-issues/injuries-emergencies/sports-injuries/Pages/Knee-Pain-and-Osgood-Schlatter-Disease.aspx
King, Christopher. Textbook of Pediatric Emergency Procedures. New York: 2008.
Martin, Sean N., DO & deWeber, Kevin, MD, FAAFP, FACSM (2016). Lateral collateral ligament injury and related posterolateral corner injuries of the knee. . In T.W. Post, K. Fields & J. Grayzel (Eds.), UptoDate. Available from https://www.uptodate.com/contents/lateral-collateral-ligament-injury-and-related-posterolateral-corner-injuries-of-the-knee?source=search_result&search=lateral%20collateral%20ligament%20injury&selectedTitle=1~19
McDonald, James, MD, MPH, FAAFP, FACSM & Rodenberg, Richard, MD (2016). Posterior cruciate ligament injury. In T.W. Post, F. OConnor & J. Grayzel (Eds.), UptoDate. Available from https://www.uptodate.com/contents/posterior-cruciate-ligament-injury?source=search_result&search=posterior%20cruciate%20ligament%20injury&selectedTitle=1~19
Orthopaedic Review. (n.d.). Retrieved January 22, 2017, from http://www.orthobullets.com/.
Therese L. Canares and Gregory Lockhart S. Sprains. Pediatrics in Review. 2013;34;47
Wolf, Michael. Knee Pain in Children, Part III: Stress Injuries, Benign Bone Tumors, Growing Pains. Pediatrics in Review Mar 2016, 37 (3) 114-119; DOI: 10.1542/pir.2015-0042. Print.
Zitelli, B., McIntire, S. C., & Nowalk, A. J. (2017). Atlas of Pediatric Physical Diagnosis. St. Louis, MO: Elsevier.
Image sources
Wikimedia Commons, the free media repository. Retrieved 14:24, June 1, 2018 from https://commons.wikimedia.org/w/index.php?title=File:Gartland_Classification.jpg&oldid=223733480.
Unless otherwise noted:
All unspecified computer graphics/drawings were created by Pablo Lopez and used with his permission.
All unspecified photographs by Sharon Sanchez, MD University of Texas Medical Branch and used with her permission.
All unspecified radiographic images were created by Leonard Swischuk MD, University of Texas Medical Branch and used with his permisson.