Fractures
Like burns and bruises, certain fracture presentations are likely to be accidental, whereas others are highly likely to be inflicted.
Accidental, uncomplicated linear fractures of the parietal bone, for instance, are commonly seen in older infants and toddlers after falls from high chairs or counter tops onto hard surfaces.
Spiral fractures occur when one end of an extremity is fixed (e.g., a foot is planted on the floor) but the rest of the extremity remains in motion. Accidental spiral fractures of the tibia are common in preschool children who fall short distances onto an extended leg, and are often called "toddler's fractures." Spiral fractures in very young children are highly suspicious for abuse since they are the result of forceful twisting or jerking of an extremity.

Fig. 19: "Toddlers fracture" (minimally displaced spiral fracture of tibia) in a 3 year old. Note periosteal new bone formation, indication this fracture is at least 7-10 days old.
Transverse fractures of long bonesare usually the result of direct impacts, and thus are more common in older children after sports injuries. When seen in younger children, the possibility of abuse should be carefully considered.

Fig. 20: Transverse fracture of the humerus in a 5 month old.
Torus or buckle fracturesare caused by axial loading on an extended extremity (e.g., a fall onto an outstretched arm or, in smaller children, a leg). They are most commonly seen in preschool children because their actively growing metaphyses have a lower tolerance for this type of loading.

Fig. 21: Torus ('buckle') fracture of the distal femur in a 7 month old who rolled off his parents' bed. No other findings of trauma after complete evaluation.
It is important to remember that certain fracture presentations are highly likely to be inflicted. (Note that the same general principles for distinguishing accidental from abusive bruises and burns also apply to fractures.)
- Any fracture in an infant under age 6 months. Very young infants have limited mobility and rarely would fall a sufficient distance to cause a fracture.
- Spiral fractures of the femur or humerus in non-ambulatory children. The most common mechanism is forceful jerking or twisting of the extremity while being held near the knee or elbow.

Fig. 22: Spiral femur fracture in a 3 month old girl. Her father claimed he was changing her diaper and "heard a pop."
- "Chip" or "corner" fractures of the metaphyses of long bones. These are also produced by forceful jerking or twisting of an extremity. These are commonly encountered in infants who have been severely shaken (see section on Abusive Head Trauma).

Fig. 23: "Chip" or "corner" fractures of distal tibia in a 4 month old girl with numerous other fractures of varying ages.
- Rib fractures (commonly encountered in shaken infants).
- Posterior rib fractures are highly specific for abuse.

Fig. 24: Multiple posterior rib fractures in an infant with abusive head trauma.
- Complex or depressed skull fractures. These are typically the result of much higher-energy and focused impacts (i.e., direct blows) than would occur in typical household falls.

Fig. 25: Complex skull fracture in an 8 month old with numerous other injuries.
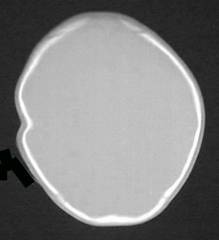
Fig. 26: Depressed skull fracture in a 1 year old child.