Abusive Head Trauma in Infants
Inflicted head trauma is the most common reason for hospital admission in abused children, and primarily affects children aged 2 years and under. As noted in the introduction, head trauma is the leading manner of death in abused children; fatal head injury is particularly common in children under age 1 year.
Most perpetrators of infant head trauma are either parents, step-parents, or paramours of the parents, and most assaults are unwitnessed. The assaults are extremely violent and, if they were witnessed, would never be mistaken for normal play with, or care for, an infant.
More info: head trauma in infants
Several factors make infants more prone to brain injury during violent assaults:
- The head is larger in proportion to the body (as compared to adults); while
- The neck muscles are less well developed, meaning that the infant's head is are more prone to rapid multidirectional jerking in response to severe shaking.
- The infant brain has a higher water content and less well-developed glial support, making it more prone to damage from shearing forces.
- The subdural space is larger in infants compared to adults, allowing for more brain motion within the skull vault and making the subdural bridging veins more susceptible to rupture in response to shearing forces.
Most cases of inflicted head trauma in small children involve some combination of severe shaking and/or violent impact. The proportion of injury caused by each mechanism varies from case to case, which makes generalization difficult, but most children present with at least three of the following four findings:
- Diffuse cerebral edema;
- Subdural hemorrhage;
- Retinal hemorrhages; and
- Fractures, particularly posterior rib fractures and metaphyseal chip fractures. Skull fractures are commonly seen after impact trauma.
Severe accidental head injuries may result in one or perhaps two of the above injuries, particularly subdural hemorrhage, but the more of the above findings are present, the more likely the head injury is to have been inflicted.
Diffuse cerebral edema
Assaults on infants that involve violent shaking, or that involve impacts with sudden deceleration (e.g., hitting an infant's head on a countertop or even brutally throwing a child against a mattress) can produce multiple and unpredictable shearing forces within the skull. These shearing forces can cause neuronal and axonal injury, rupture, or death. Cytokines and other inflammatory mediators released by the injured neurons begin a cascade of secondary effects that, within minutes to hours, produce severe cerebral edema. A combination of hypoxia at the cellular level resulting from this inflammatory cascade, and apnea or hypoventilation accompanying the altered level of consciousness often produces hypoxic-ischemic injury that may be the most prominent finding on brain imaging studies.
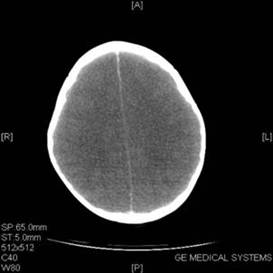

Fig. 28: Diffuse cerebral edema in a 2 year old with subdural hematoma and retinal hemorrhages. Note loss of grey-white matter distinction and compression of extra-axial spaces. Compare with CT scan on right: obtained in a 5 month old with scalp contusion but no CNS injury. Note the prominent ventricles and extra-spaces and good grey-white matter differentiation in frontal lobes.
Cerebral edema in severely abused infants is usually generalized, and reflects the global insult to the brain caused by shaking or high-energy impact. Localized brain edema is less common and is more likely the result of a single sharp blow to the head.

Fig. 29: Impact subdural hematoma (arrow) and ipsilateral cerebral edema in an infant.

Fig. 30: Scalp contusion (arrow) epidural hematoma and mild focal cerebral edema from focal trauma to right frontal area. Note the otherwise normal brain and surrounding spaces.
Subdural hemorrhage
Subdural bleeding results from rupture of bridging veins traversing the extra-axial space between the brain and the major venous sinuses. Infants are more prone to subdural bleeding because their extra-axial spaces are wider than in adults, making their veins more likely to break with translational movements of the brain within the cranial cavity during major trauma.
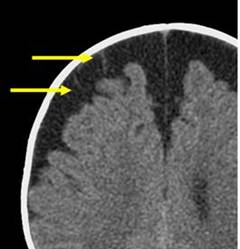
Fig. 31: Infant with normally large subarachnoid spaces (referred to as Benign Extra-axial Fluid Collections of Infancy). Subdural bridging veins can be clearly seen traversing the right frontal subarachnoid space (arrows).
In most cases the amount of blood lost in subdural hemorrhages is not extensive; mass effects on the brain or anemia from blood loss is unusual. The significance of the subdural bleeding is not its volume but its indication of the type and amount of force to which the brain has been subjected.

Fig. 32. Photo from autopsy of 4 month old infant who died of abusive head trauma. Subdural hemorrhage is visible at top left (arrow). Diffuse cerebral edema is also noted (brain is overflowing out of the cranial vault).
Retinal hemorrhage
Retinal hemorrhages are encountered in approximately 80% of cases of severe abusive head trauma, and are only seen in 5 to 10% of infants with severe accidental head trauma. The most likely mechanism for production of the widespread, multilayered retinal and preretinal hemorrhages characteristic of inflicted head injury in infants is related to the observation that the vitreous humor is more closely adherent to the retina in small children than in adults. Thus, in response to shaking or other trauma producing violent rotational movements of the eyes, the vitreous humor exerts extreme traction on the retina, producing widespread hemorrhage. In contrast, even extreme unidirectional trauma (e.g., a head impacting a dashboard in an auto accident) most commonly causes either no retinal hemorrhages, or at most a few small hemorrhages close to the optic nerve head.

Fig. 33: Widespread retinal and preretinal hemorrhages in a 4 month infant who died of abusive head trauma (same case as Fig. 32)