Left-to-Right Shunts
The flow through the systemic and pulmonary circulations is normally balanced and equal in volume (Qp/Qs =1). The two circulations are placed in series with each other. The same volume of blood first makes its way through the systemic circulation, then the pulmonary circulation, then back to the systemic circulation, and so on.
Left to right shunts are characterized by a "back-leak" of blood from the systemic to the pulmonary circulation. This causes the pulmonary flow to be larger than the systemic flow (Qp/Qs >1). As a consequence, the pulmonary circulation carries not only the blood that entered the right atrium and right ventricle through the superior and inferior vena cava, but also the additional blood entering through a VSD, ASD, AVSD or PDA. Blood volume and/or pressure in the pulmonary circulation become abnormally high. If the shunt is significant, there is progressive damage to the pulmonary vasculature and gradual development of irreversible pulmonary hypertension. The pressure in the pulmonary circuit may ultimately exceed the systemic pressure causing reversal of blood flow from the right side of the circulation to the left (Eisenmenger syndrome). This may take as short as 1-2 years in a large VSD, AVSD, or PDA, or as long as a few decades as in ASD.
Lesions resulting in left-to-right shunts include:
- Ventricular septal defect (VSD)
- Patent ductus arteriosus (PDA)
- Atrial septal defect (ASD)
- Atrioventricular defect (AVSD)
In small (restrictive) VSD and PDA, the direction and magnitude of the shunt depends on the pressure difference across the shunt. In large VSD and PDA, the direction and magnitude of the shunt depends on the relative resistance in the pulmonary and systemic circuits.
In ASD, the magnitude of the shunt depends largely on relative ventricular compliance (elasticity).
AVSD is a mix between ASD and VSD depending on the predominant lesion.
The defect size is determined by comparing its diameter with the aortic annulus. A small defect is less than 1/3 of the aortic annulus. A moderate sized defect is 1/3 to 2/3, and a large defect is >2/3 the size of the aortic valve annulus.
Ventricular Septal Defects (VSD)
Isolated ventricular septal defects (VSDs) constitute 25-30% of all congenital heart diseases (CHD) in children. VSD may be present in 50% of CHDs such as in Tetralogy of Fallot, double outlet right ventricle, truncus arteriosus and others.
Types
- Membranous
- Muscular
- Inlet (usually a part of AV canal defect)
- Outlet (Supra-cristal, sub-arterial)
Anatomy
Approximately 70% of all VSDs are present in the membranous portion of the inter-ventricular septum, about 20% are in the muscular portion, and the remaining defects are at either the inlet or the outlet portions of the ventricular septum. The inlet VSD is usually a part of atrioventricular septal (AV canal) defect. The outlet (supra-cristal) VSD is more common (about 20%) in the oriental population (or East Asian population).
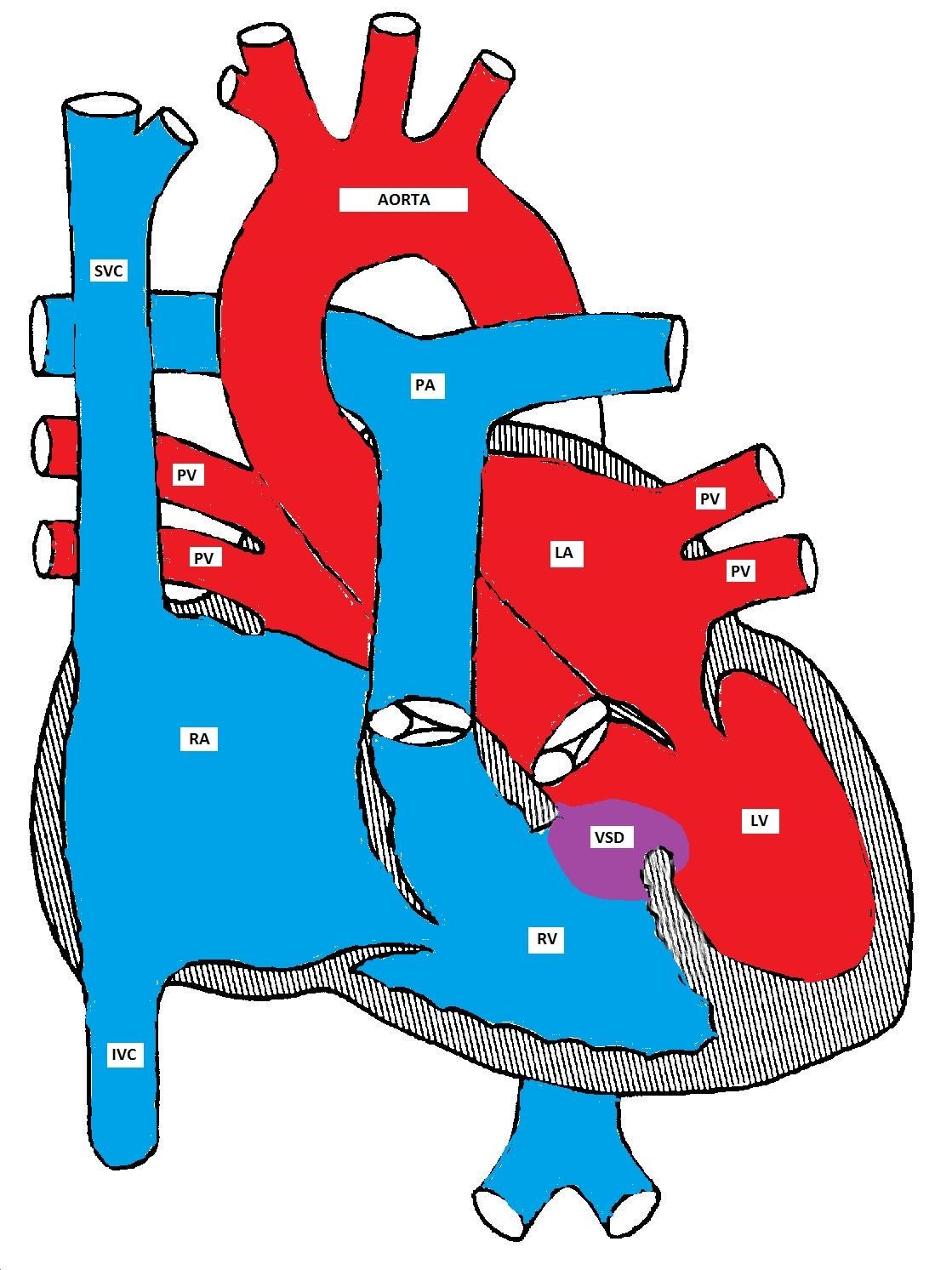
A ventricular septal defect
Pathophysiology
With a small sized VSD, "restrictive VSD," the direction and magnitude of the shunt depends on the size of the VSD and the pressure gradient between the left and right ventricles. The restrictive nature of the VSD maintains the pressure gradient between the two ventricles.
With a large VSD, the hole is not restrictive and the pressure in both ventricles is almost equal. The direction and magnitude of the shunt depend on the relative difference between the pulmonary and the systemic vascular resistances. In fetal life, the pulmonary resistance is higher than the systemic resistance. As the lungs expand with the first breath, the pulmonary resistance drops significantly and the pulmonary flow increases. The pulmonary resistance continues to decrease until reaching the normal adult ratio of 1:10 by 4-8 weeks (see figure).
Prolonged large left-to-right shunt leads to gradual increase in the pulmonary pressure and pulmonary hypertension eventually develops. As the pressure difference between the systemic and pulmonary systems decreases, the flow across the shunt also decreases. If the pulmonary vascular resistance exceeds the systemic vascular resistance, the direction of the shunt reverses and cyanosis develops (Eisenmenger syndrome). This may develop within two years in otherwise healthy kids and within one year in patients with Down's syndrome.
The drop in pulmonary vascular pressure/resistance and the increase in pulmonary blood flow after birth
Clinical Presentations
Children with a small VSD are usually asymptomatic. An incidentally discovered holosystolic or decrescendo heart murmur is the most common presentation. The murmur is commonly discovered shortly after birth as the pulmonary vascular resistance drops and the pressure difference between the two ventricles becomes remarkable. The intensity of the murmur is inversely proportional to the size of the VSD because of the increased turbulence and flow velocity produced by a smaller defect. A thrill may be palpable in some cases. The defect may be small enough to almost close at the end of a systolic decrescendo murmur.
An infant with a large VSD may be asymptomatic in the first few days/weeks of life until the pulmonary vascular resistance drops. As the pulmonary resistance decreases, the left-to-right shunt increases. The right ventricle is thus subjected to high pressure and becomes hypertrophied while the left atrium and left ventricle receive more volume and become dilated. The right atrium is not usually affected. Congestive heart failure (CHF) may develop and presents as tachycardia, tachypnea, exertional dyspnea, breathlessness and sweating during feeding. The child's growth is also often delayed because of poor caloric intake. In some infants, especially those with Down's syndrome, the pulmonary vascular resistance may not significantly drop. These infants may not develop CHF but are at increased risk of developing pulmonary hypertension. They may need earlier surgical intervention to prevent worsening of pulmonary hypertension and the early development of Eisenmenger syndrome.
Making the Diagnosis
|
|
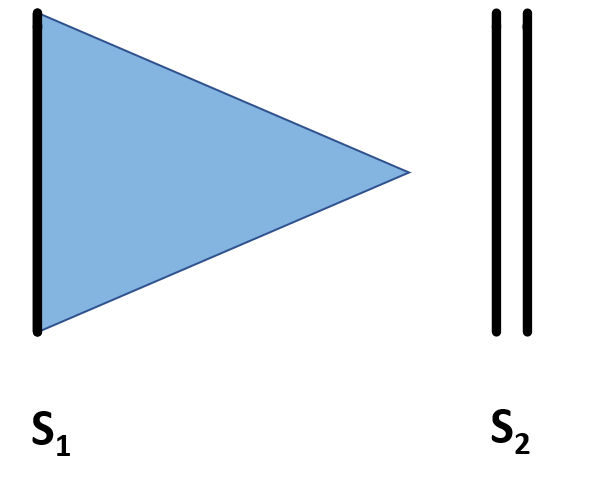
A Holosystolic murmur is heard at the left sternal border due to turbulent flow across the VSD. The intensity of the murmur is inversely proportional to the magnitude of the shunt; the smaller the shunt, the louder the murmur and vice versa.
|
|
|
A decrescendo (early) systolic murmur may indicate a small and closing VSD. There is diminished flow in the latter part of systole and no murmur is heard.
|
|
|
An apical mid-diastolic murmur (rumble) may be heard due to increased flow across the mitral valve (relative mitral stenosis). This indicates that the VSD is large enough to cause excessive pulmonary blood flow and this clinically indicates congestive heart failure (CHF). This CHF is not due to pump dysfunction as in adults but due to the increased pulmonary blood flow.
|
|
|
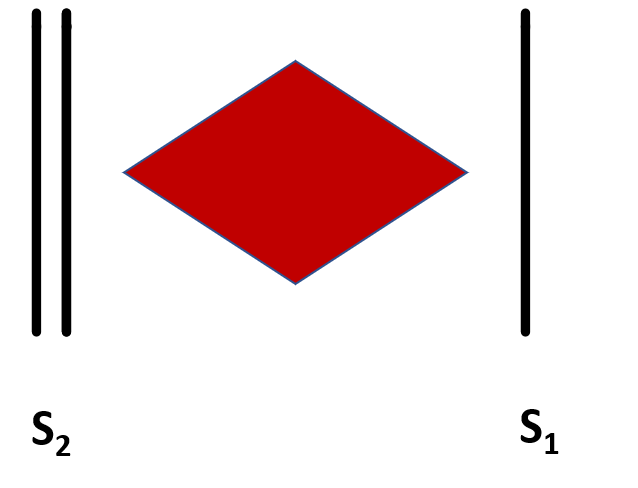
An early diastolic murmur heard at the upper left sternal border in a sitting position could be heard in a small membranous or a supra-cristal VSD. This indicates aortic insufficiency due to prolapse of one of the aortic valve cusps into the VSD secondary to the suction created by the high velocity jet (Venturi effect).
|
|
|
An early diastolic murmur may also be heard in older children due to pulmonary insufficiency if pulmonary hypertension develops. In that case, the second heart sound may be loud and narrowly split.
|

- Pulmonary hypertension diminishes the pulmonary blood flow and makes CHF unlikely (honeymoon before the development of Eisenmenger syndrome).
- Cardiomegaly and hepatomegaly may be present if CHF is present.
- Chest radiographs may show cardiomegaly and increased pulmonary vascularity.
- EKG reflects the hemodynamic status and may show RVH, left atrial enlargement and left ventricular enlargement, (the EKG is not very sensitive in differentiating LVH from LV dilation). The right atrium is usually unaffected.
- Echocardiogram shows the location, type and size of the VSD. It can also estimate the pressure gradient across the VSD. The hemodynamic effects of VSD on different chambers can be elucidated. It is also important to look for aortic insufficiency (especially in membranous and supra-cristal VSD) which may indicate an early damage to the aortic valve.
- Cardiac catheterization is rarely needed but could measure the pulmonary pressure/resistance and help to determine the reactivity (and hence operability) of the pulmonary vasculature in case of pulmonary hypertension
Natural History
While more than half of small and medium sized VSDs close spontaneously, only about 10% of large VSDs close spontaneously. The muscular VSD closes by muscle in-growth. The membranous VSD closes by the neighboring tricuspid valve leaflet tissue. This forms an aneurysm that gradually gets endothelialized. Both inlet and supra-cristal (outlet) VSDs are unlikely to close spontaneously. In unoperated patients with large VSD, Eisenmenger syndrome may develop within two years but may develop as early as one year in Down syndrome patients. This could be attributed to the decreased vascular/alveolar density and increased secretion of endostatin in Down syndrome patients.
Management
Asymptomatic children with a small or medium sized VSD need only supportive care, with the expectation that the VSD will close in the first few years of life. If CHF develops, treatment consists of diuretics, afterload reducing agents such as ACE inhibitors, and possibly digoxin. Heart failure in left-to-right shunts is due to volume overload to the pulmonary circulation. This is in contrast to adults with myocardial infarction in which heart failure is due to pump dysfunction. In adults with heart failure, digoxin is used to enhance pump function. However, if digoxin is used in treatment of CHF due to left-to-right shunt, it works primarily for its cholinergic effect to decrease the heart rate. Fluid restriction should be avoided as it reduces the caloric intake and delays growth.
Oxygen therapy should also be avoided. It is a pulmonary vasodilator and a systemic vasoconstrictor that would worsen the left-to-right shunt and CHF symptoms. Patients with persistent CHF or those who are developing pulmonary hypertension require surgical closure of the VSD. If a patient is not a suitable candidate for surgery, pulmonary artery banding should be considered until surgery can be done (usually within the first year of life). Recently trans-catheter techniques have been used to close VSDs (especially the muscular VSDs).
Patent Ductus Arteriosus (PDA)
Anatomy
The ductus arteriosus, formed from the embryonic 6th aortic arch, connects the aorta to the pulmonary artery. It normally closes within a few days after birth. A high oxygen tension and a decrease in endogenous prostaglandins are important factors in inducing ductal closure. For the same reason, prostaglandin synthetase inhibitors, such as indomethacin, are effective in inducing ductal closure and are commonly used in the neonatal period, especially in preterm infants.
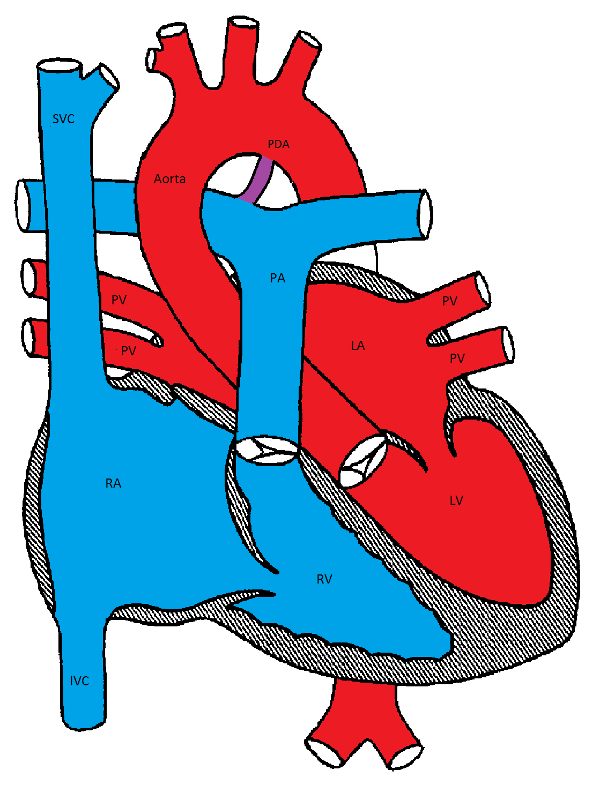
Patent Ductus Arteriosus
Pathophysiology
Failure of closure of the ductus arteriosus leads to hemodynamic changes similar to those seen in VSD. The direction and extent of the shunt in the PDA depends on the size of the PDA and the relative systemic and pulmonary vascular resistances.
Clinical Presentations
PDA is more common in females, premature infants, patients with Down Syndrome and congenital rubella syndrome. The symptoms are similar to those found in VSD and depend on the size of the shunt and direction of flow. While a small PDA is usually asymptomatic, a large PDA with significant left-to-right shunt may lead to CHF and eventually pulmonary hypertension.
Making the Diagnosis
- In older children, PDA classically produces a continuous or "machinery" murmur due to flow across the shunt throughout the cardiac cycle. In newborn infants, especially those born prematurely, the murmur may be heard only during systole because the higher pulmonary arterial pressure diminishes flow during diastole.
- An apical mid-diastolic murmur may be heard because of increased flow through the mitral valve (relative mitral stenosis). This usually signifies a large PDA and is often associated with CHF.
- Wide pulse pressure indicates a large left-to-right shunt due to a sudden drop in diastolic pressure.
- In a small PDA, the EKG is usually normal. In a large PDA, the EKG will demonstrate right ventricular hypertrophy, left ventricular enlargement, and left atrial enlargement, due to volume overload.
- Chest radiographs may show increased pulmonary vascularity and cardiomegaly due to left atrial and left ventricular enlargement. The heart size might be normal if the shunt is small.
Natural history and management
Small and moderate sized PDA often close spontaneously especially, in full term infants. PDA in premature infants may need indomethacin treatment (in the first 2-4 weeks of life) or surgical ligation. Transcatheter device closure of PDA is commonly used in older children.
Atrial Septal Defects (ASDs)
Anatomy
Atrial septal defects involve many different parts of the atrial septum. The septum secundum defect is the most common and comprises 6-10% of all CHD. It is located in the fossa ovalis, in the location of the foramen ovale. The primum septal defect is considered a partial form of atrioventricular septal defect. The other "less common" types of ASDs are the sinus venosus and the unroofing of the coronary sinus.
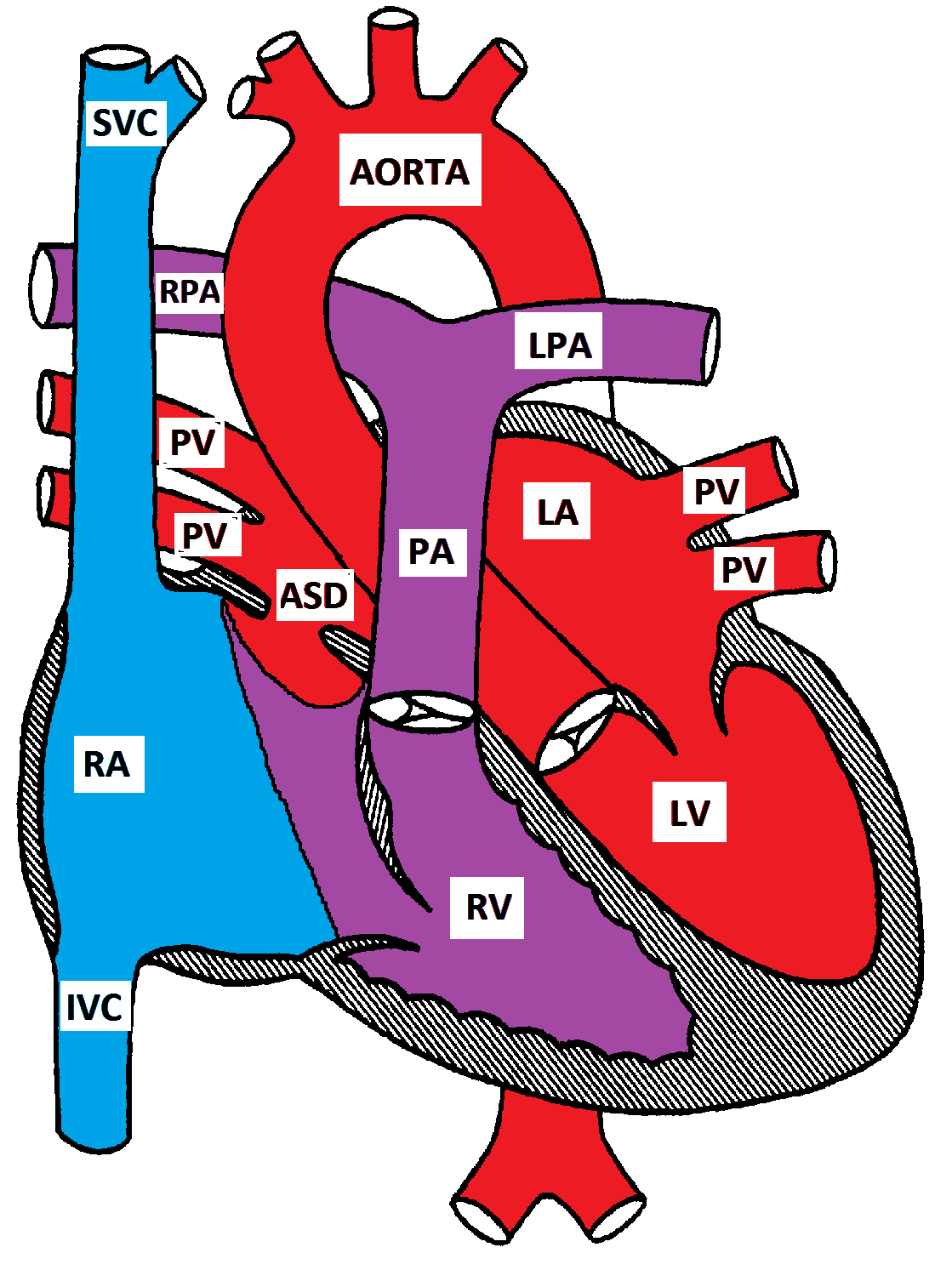
Secundum Atrial Septal Defect
Pathophysiology
Since the pressure difference between the two atria is small, no turbulence is generated by the flow across the ASD. In moderate to large ASDs, the direction and magnitude of the shunt across the ASD depends on the relative right and left ventricular compliances. In early infancy, the right ventricular compliance is low and the shunt across the ASD is small. As the right ventricular compliance increases, the left-to-right shunt increases. If the right ventricular compliance decreases, later in life, the shunt decreases. The shunt may eventually reverse if the patient develops pulmonary hypertension and Eisenmenger syndrome. This usually takes a few decades to develop.
Clinical Presentation
ASD is usually asymptomatic and typically presents with a heart murmur in preschool age. CHF rarely develops in patients with a large ASD. Right atrial stretch may cause atrial arrhythmias. Prolonged volume overload of the lungs eventually causes pulmonary hypertension, which may take 4 to 5 decades to develop.
Making the Diagnosis
- No murmur develops due to the flow across the ASD since there is only a minimal pressure gradient between the two atria and no turbulence is generated.
- A systolic ejection murmur may be heard in the pulmonary area due to increased flow across the pulmonary valve (relative pulmonary stenosis).
- A mid-diastolic murmur may be heard at the lower left sternal border due to increased flow across the tricuspid valve. This murmur is rarely heard because the tricuspid valve annulus is bigger than the pulmonary valve annulus. A tricuspid valve murmur indicates that the patient is in CHF due to a large left-to-right shunt.
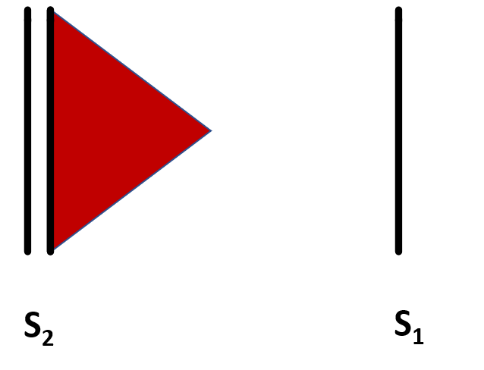
- A wide splitting of S2 is due to delayed closure of P2 secondary to increased flow across the pulmonary valve.
- The splitting of S2 is "fixed" and does not vary with respiration. This is due to diminished effects of respiratory cycle on the right ventricular volume. In inspiration, the venous return to the right atrium increases and impedes the left-to-right shunt across the ASD. In expiration, the venous return to the right atrium decreases and the shunt across the ASD increases. In both cases, the volume of blood in the right ventricle is increased and remains unchanged in both inspiration and expiration.
- EKG may demonstrate right atrial enlargement, right ventricular conduction delay (incomplete right bundle branch block), right ventricular dilation, and right axis deviation.
- Chest radiograph shows increased pulmonary vascularity, right atrial and right ventricular enlargement.
- Echo cardiogram is diagnostic
Management
Most patients with ASD are asymptomatic and no specific medical management is necessary. Medical management (as in VSD) may be needed if CHF is present. Trans-catheter closure is the preferred method of closing the secundum ASDs. Surgical closure may be needed in patients with a large secundum ASD could not be closed by a trans-catheter device. Other tytpes of ADS are unlikely to close spontaneously and may need surgical closure.
|
|
ASD |
VSD |
|---|---|---|
|
Age at Presentation |
1-4 years |
2-4 weeks |
|
Gender Predominance |
Females |
Males |
|
Epidemiology |
10% of all CHD |
25% of all CHD |
|
Associated conditions |
Mutations in TBX5 gene (Holt-Oram syndrome), GATA4 gene, and MYH6 gene; Treacher Collins syndrome, Noonan syndrome |
Thrombocytopenia absent radius syndrome, Apert syndrome, Cru-di-chat syndrome, Trisomy 21 |
|
Types |
Secundum, primum, sinus venosus, unroofed coronary sinus |
Perimembranous, muscular, inlet, outlet |
|
Murmurs |
SEM: pulmonary overflow Mid-diastolic: tricuspid overflow |
Holosystolic: turbulence across VSD |
|
Intensity of Murmur |
Increases with increased size due to increased flow over the pulmonic valve |
Decreases with increased size due to decreased turbulent flow |
|
Determinant of Shunt |
Small ASD: atrial pressure difference Large ASD: relative ventricular compliance |
Small VSD: relative ventricular pressures |
|
Symptoms |
- Usually asymptomatic - If symptomatic, typically presents with exercise intolerance - CHF is rare (presents at 9-12 months with decreases activity tolerance, dyspnea, FTT) - Arrythmias (presents at 4th-5th decade of life, most common presenting symptom) - Eisenmenger syndrome (presents at 5th-6th decade of life) |
- May be asymptomatic - CHF (presents at 4-8 weeks with difficulty feeding, dyspnea, FTT) - Eisenmenger syndrome (presents at ~2 years) |
|
Examination |
Murmurs, wide fixed S2, RV impulse at LLSB |
Murmurs, dynamic precordium |
|
EKG findings |
RAE, RAD, RVH, incomplete RBBB |
RVH, LAE, LVH |
|
Effects on Cardiac Chambers |
RA dilation, RV dilation |
RV hypertrophy, LA dilation, LV dilation
|
|
Management |
- Supportive care - Closure if necessary |
-Supportive care if asymptomatic - If symptomatic: - Increased caloric intake - Diuretics, ACE inhibitors if in CHF - Closure at 6-9 months if no longer responding to medical management |
Atrioventricular Defect (AVSD)
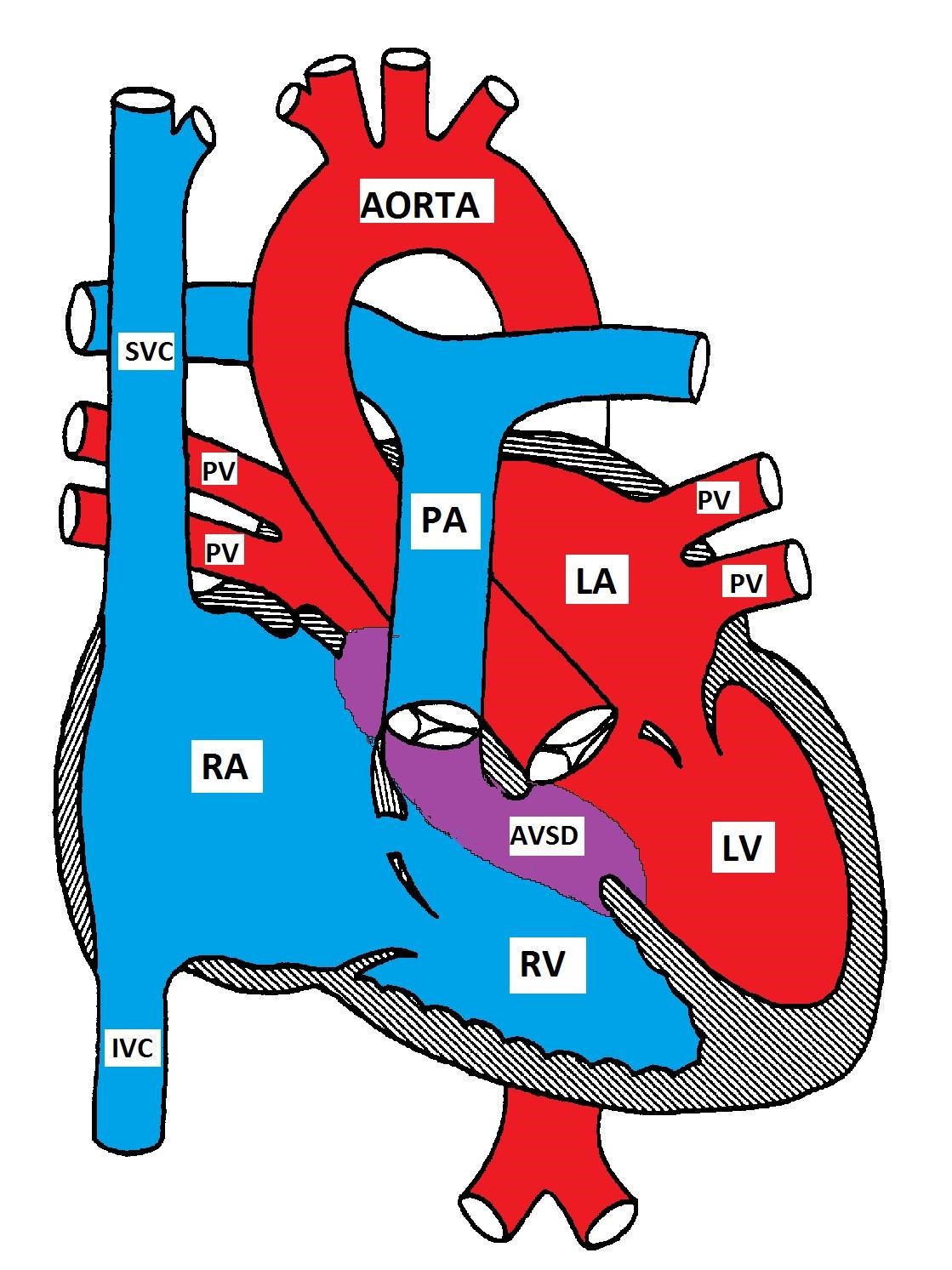
Atrioventricular Septal Defect
AVSD occurs in 2% of all CHD and is more prevalent in patients with Down Syndrome. Forty percent of children with Down syndrome have CHD and 40 % of the defects are forms of AVSD
Anatomy
Atrioventricular septal defect is also known as endocardial cushion defect (ECD) and atrioventricular canal (AVC). It consists of a variety of defects in the endocardial cushions which form the lower part of the atrial septum, upper part (inlet) of the ventricular septum, and the medial parts of the AV valves.
There are 4 possible types:
a) Partial AVSD (primum ASD) consists of a defect in the lower part of the atrial septum and is usually associated with a cleft in the anterior mitral leaflet causing mitral insufficiency. The ventricular septum is usually intact.
b) Complete AVSD has a defect that extends from the lower part of the atrial septum to the upper part (inlet) of the ventricular septum. The mitral and tricuspid valves lose their anchor points in the ventricular septum and are instead attached to each other, forming a common AV valve that overhangs the ventricular septum.
c) Intermediate AVSD is similar to the complete AVSD but has two AV valves with a primum ASD and a large inlet VSD.
d) Transitional AVSD is similar to the intermediate AVSD but the VSD is small.
Pathophysiology
The pathophysiology depends on the predominant lesion (atrial vs ventricular). There is a left-to-right shunt at the atrial level due to increased relative right ventricular compliance leading to right atrial enlargement. Left atrial enlargement occurs because of mitral insufficiency secondary to the mitral valve cleft. There is a varying degree of pulmonary hypertension as the pulmonary vasculature is exposed to excess blood volume at higher pressures. Pulmonary hypertension may develop in the first two years in normal patients and in the first year in patients with Down's syndrome.
Clinical Presentations
The clinical presentation of AVSD is variable and depends on the size of the defect and the degree of the left-to-right shunt. Patients with complete AVSD usually present with congestive heart failure in the first few weeks of life, while those with partial AVSD (primum ASD) may be completely asymptomatic.
Symptoms of CHF include poor feeding, shortness of breath, diaphoresis during feeding, and poor weight gain. Mild cyanosis may rarely develop because of right to left shunt due to increased pulmonary resistance or due to preferential streaming of the venous blood from the IVC to the left atrium.
Making the Diagnosis
- Physical findings are variable and depend on the presence or the absence of congestive heart failure. The precordium may be hyper-dynamic and the cardiac apex may be displaced inferiorly and to the left.
- The auscultatory findings are also variable and may include a systolic ejection murmur due to increased flow through the pulmonary valve with wide and fixed splitting of S2 as in ASD. A loud, single S2 indicates pulmonary hypertension.
- Additional auscultatory findings include a mid-diastolic murmur at the lower left sternal border due to increased flow through the tricuspid valve, apical holosystolic murmur radiating to the left axilla due to mitral insufficiency, and a holosystolic murmur of VSD.
- EKG is characterized by left superior axis deviation due to inferior and posterior displacement of the AV node (anatomical). It may also show right ventricular hypertrophy (due to increased pressure), right atrial enlargement, and LVH. A prolonged PR interval (first degree heart block), probably due to abnormal AV node conduction, may be present.
- Chest radiograph shows varying degrees of cardiomegaly and increased pulmonary vascularity.
- Echocardiography is useful in demonstrating the anatomical lesions and associated abnormalities. It is essential to assess the integrity of the AV valves.
Left superior QRS axis deviation (negative in avF) and right ventricular hypertrophy in AVSD
Management
CHF, if present, is managed with diuretics, ACE inhibitors, and occasionally digoxin. A high caloric-density formula should be used with no fluid restriction.
Almost all patients with AVSD will need surgery. The timing of surgery depends on the size of the patient, the presence of CHF, response to medical management, and the presence or absence of pulmonary hypertension. In asymptomatic patients with partial AVSD, surgery may be delayed until preschool age. Corrective surgery is usually performed in symptomatic patients with intractable CHF in the first few months of life. Even in patients who respond to medical management, the presence of Down Syndrome necessitates early surgery to prevent the development of pulmonary hypertension. If surgery cannot be performed in a symptomatic patient, pulmonary arterial banding may help limit the pulmonary blood flow until surgical repair is possible.
Quick Checks
![]()
