Upper Extremity Injuries
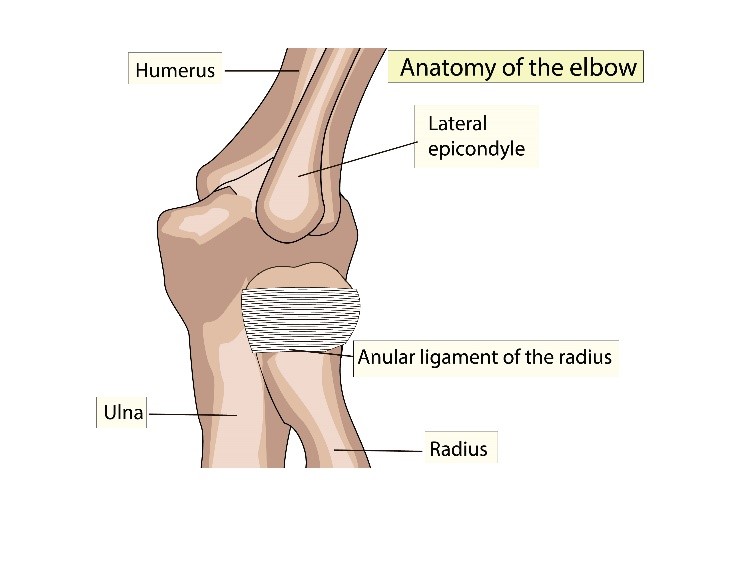
Nursemaid's Elbow (Subluxation of the Radial Head)
This injury is most commonly seen in children 3-5 years of age and rarely occurs after seven years of age. The lack of ossification of the proximal radial epiphysis in children less than five years of age make it more pliable and prone to slippage of the annular ligament.
Mechanism of Injury
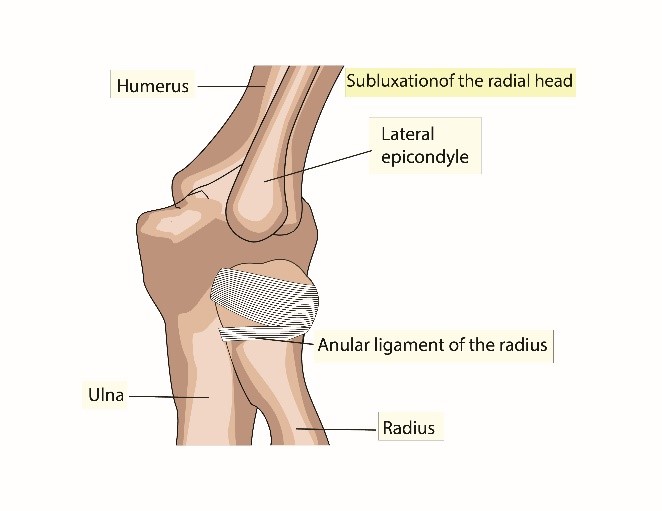
Injury is caused by longitudinal traction applied to pronated forearm and extended elbow (e.g. Child lifted or swung by the forearm). This results in subluxation of the radial head and interposition of the annular ligament into the radiocapitellar joint.
|
|
|
Physical Examination
Initial pain subsides rapidly but child is reluctant to use the arm, choosing to keep it close to the body with elbow slightly flexed and forearm pronated. Any attempt to supinate the arm causes pain. Pain and tenderness to palpation of the lateral aspect of the elbow (around the radial head and annular ligament).
Evaluation: Imaging
X-rays are not routinely indicated with a reliable history consistent with physical exam. If X-rays are done, anteroposterior and lateral views are usually normal; many times the subluxation is reduced inadvertently when technician supinates the arm to take x-rays. If the history is inconsistent, suggestive of a possible compounding injury, or if there is noticeable significant swelling of the joint or surrounding soft tissue, obtain X-rays prior to attempting reduction.
Management
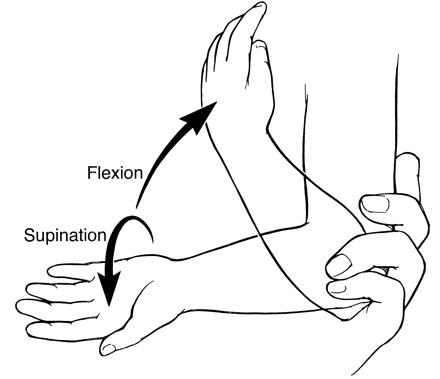
Two techniques for closed reduction (see image below). An audible or palpable click is associated with high probability of successful reduction. Child is able to use arm normally thereafter. If a definite snap or pop is not felt or if the patient fails to use the extremity, obtain x-rays if not yet done, and re-examine the entire extremity again carefully.
 |
|
|
Supination-Flexion Technique Place thumb over radial head and apply pressure. Manually supinate the arm and flex maximally - ideally past 90 degrees of flexion. |
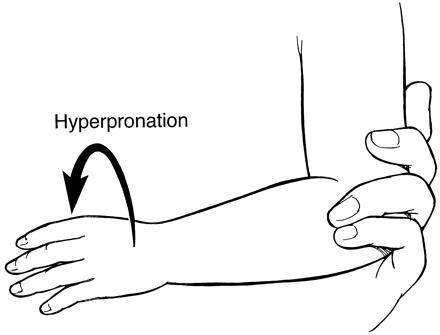
Forced Pronation Technique Hold arm flexed 90 degrees at the elbow and hyperpronate at the wrist.
|
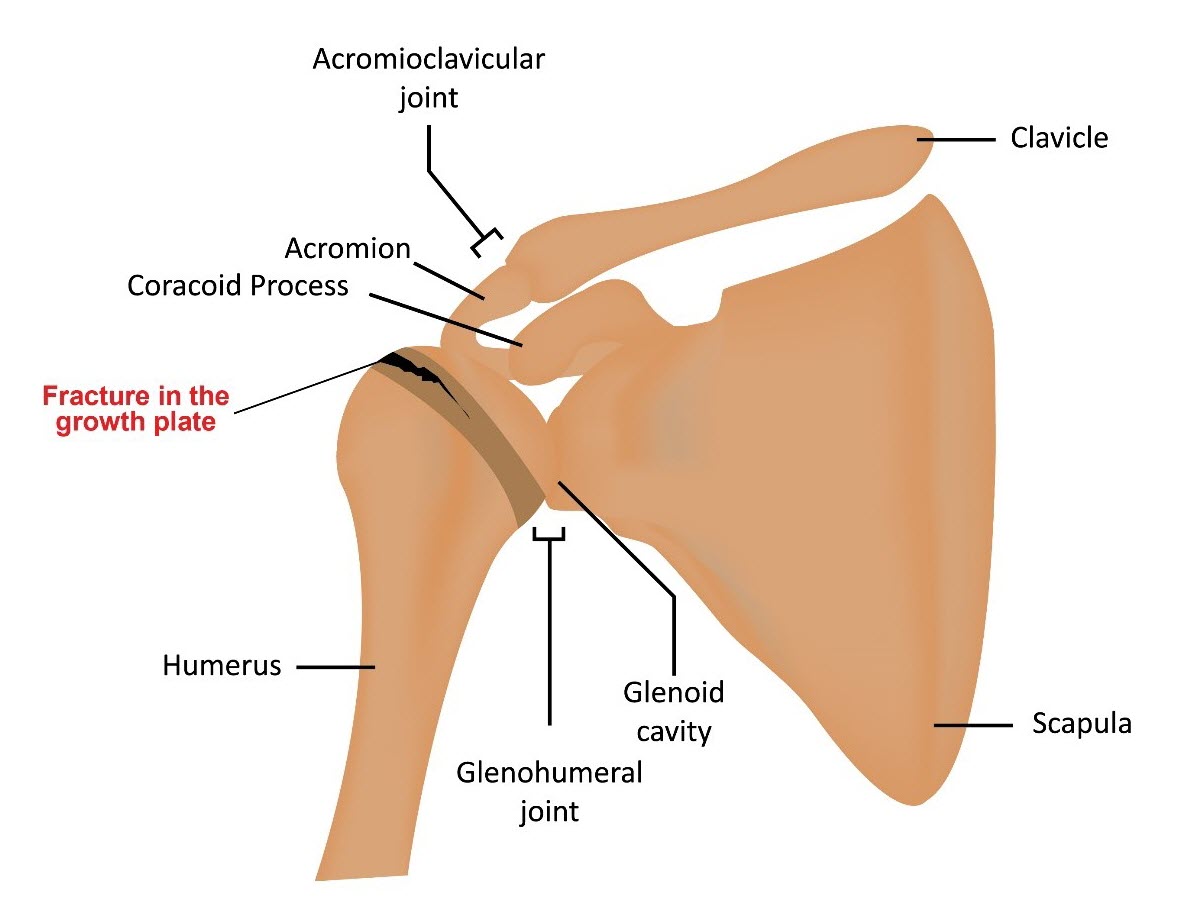
Little Leaguer's Shoulder
This condition is seen mostly in adolescent pitchers or tennis players. Typically, patients present with pain when throwing but may also present with decreased velocity and control.
Mechanism of Injury
Overuse injury is caused by overhand pitching without proper rest, pitching/throwing without proper technique, or lack of muscle strength of the shoulder and upper back. Microtrauma at the physis (Salter Harris Type 1) of the proximal humerus can also occur. There is widening of the growth plate that result in pain and swelling at the shoulder joint.
Physical Examination
Point tenderness over the shoulder physis and reproducible pain with shoulder rotation
Evaluation: Imaging
- X-ray: widened or irregular proximal humerus physis but may also be unremarkable
- MRI provides a more detailed image of both bone, growth plate and soft tissue. MRI may also be helpful to rule out other pathology.

Management
- Rest - advise to refrain from pitching from 1-3 months. May return to play when patient is asymptomatic.
- Physical Therapy - focuses on rotator cuff strengthening as well as muscles of the arms. Strength of the core, legs and hips will also enhance stability and ability to throw.
- Ice - helps with acute swelling and pain in the shoulder.
- Throwing Program - progressively increases the force and demand on the arm and shoulder until able to return to competitive play with enforcement of pitch counts:
|
Little League Baseball Pitch Count Regulations |
||
|---|---|---|
|
Age |
Limits Per Game |
Rest Requirements |
|
17-18 years |
105/day |
76 or more pitches -> 4 days rest 61-75 pitches -> 3 days rest 46-60 pitches -> 2 days rest 31-45 pitches -> 1 day rest 1-20 pitches -> 0 days rest |
|
15-16 years |
95/day |
|
|
13-14 years |
95/day |
66 or more pitches -> 4 days rest 51-65 pitches -> 3 days rest 36-50 pitches -> 2 days rest 21-35 pitches -> 1 day rest 1-20 pitches -> 0 days rest |
|
11-12 years |
85/day |
|
|
9-10 years |
75/day |
|
|
7-8 years |
50/day |
|
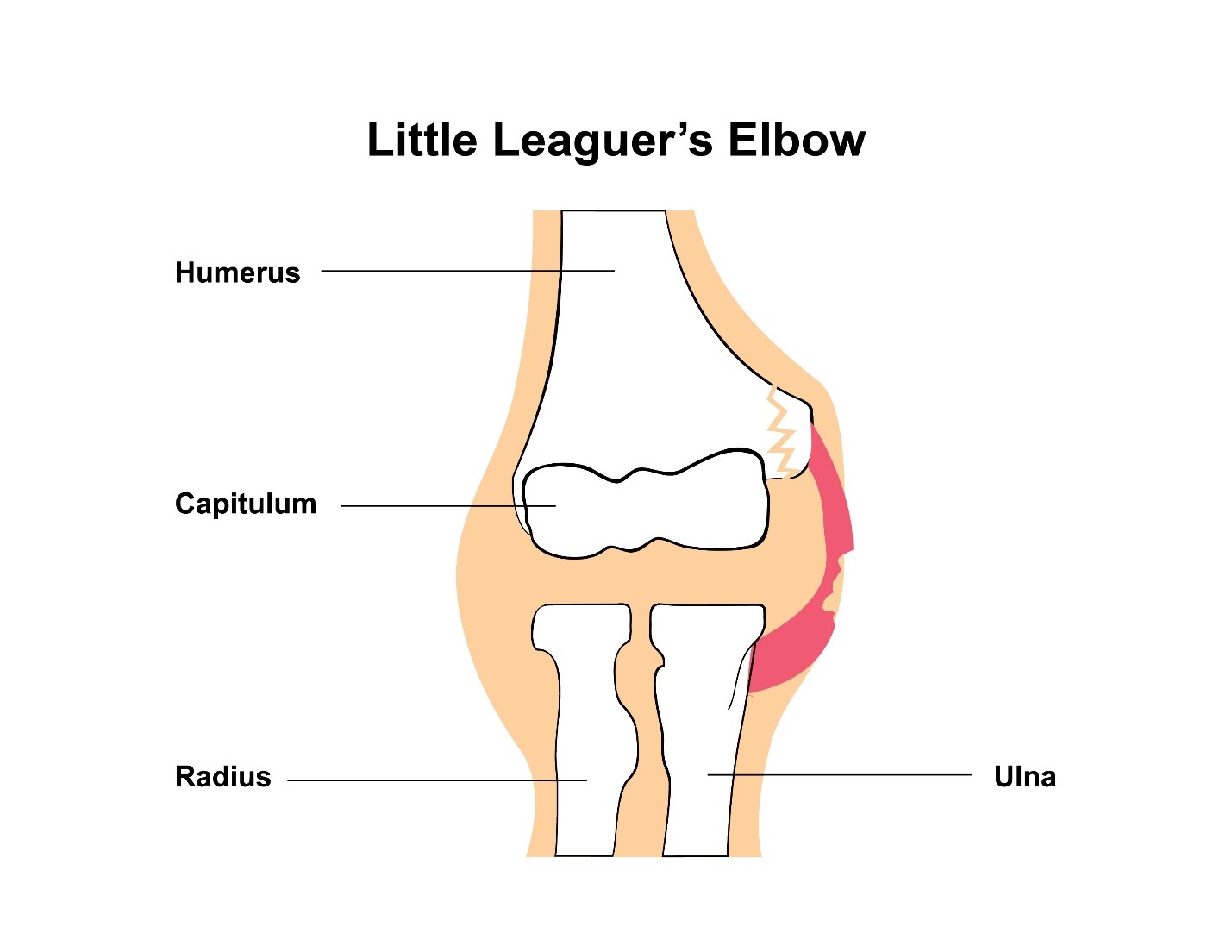
Little Leaguer's Elbow (Medial Apophysitis)
Apophysitis is defined as irritation of a bony protuberance that is a site of tendon or ligament attachment. Little leaguer's elbow is more commonly seen in active, growing children and adolescents. It is related to overuse in skeletally immature baseball pitchers (e.g. Excessive amount of pitches per game, excessive fastball speed, and continued pitching in spite of fatigue). This is a spectrum of injuries to the medial aspect of the elbow (due to excessive tension on medial epicondyle) with secondary tendinitis. The child typically develops decreased speed, accuracy and distance of pitches.
Mechanism of Injury
Injury is often associated with throwing curve balls. The excessively strong pull on the tendons and ligaments of the elbow cause repetitive microtrauma to the immature skeleton.
Physical Examination
Patient typically presents with a decrease in elbow extension. There is significant pain and swelling over the medial epicondyle accentuated by valgus stress to the elbow in extension.
Evaluation: Imaging
- X-ray: recommended AP/lateral view of elbow. X-ray may show widening or irregularity of the physeal line. X-ray may also show fragmentation or avulsion of the medial epicondyle. Chronic injury may show hypertrophy of the distal humerus with accelerated bone growth (bone age > chronological age).
|
|

- MRI may show increased edema of the medial epicondyle apophysis. MRI is most helpful to identify ulnar collateral ligament (UCL) disruption.
Management
- Non-operative
Rest - Return to play is done only when asymptomatic
Physical Therapy - focuses on arm and forearm strengthening
Ice - to help with acute swelling and pain in the shoulder
Throwing Program - progressively increases the force and demand on the arm and shoulder until able to return to competitive play with enforcement of pitch counts
- Operative: Open reduction, internal fixation (ORIF) of medial epicondyle for avulsion fractures. UCL reconstruction for UCL disruption.
Clavicular Fracture
Clavicular fractures is often seen in young, active patients. It is also the most common site of all obstetrical fractures (eg. LGA infants and those requiring instruments or special maneuvers for delivery). Associated injuries may include the scapula, the ribs, the lung (pneumothorax) and even the neurovasculature.
Mechanism of Injury
- Fall directly onto the shoulder
- Insult applied directly to the clavicle
- Occasionally caused by falling on an outstretched arm
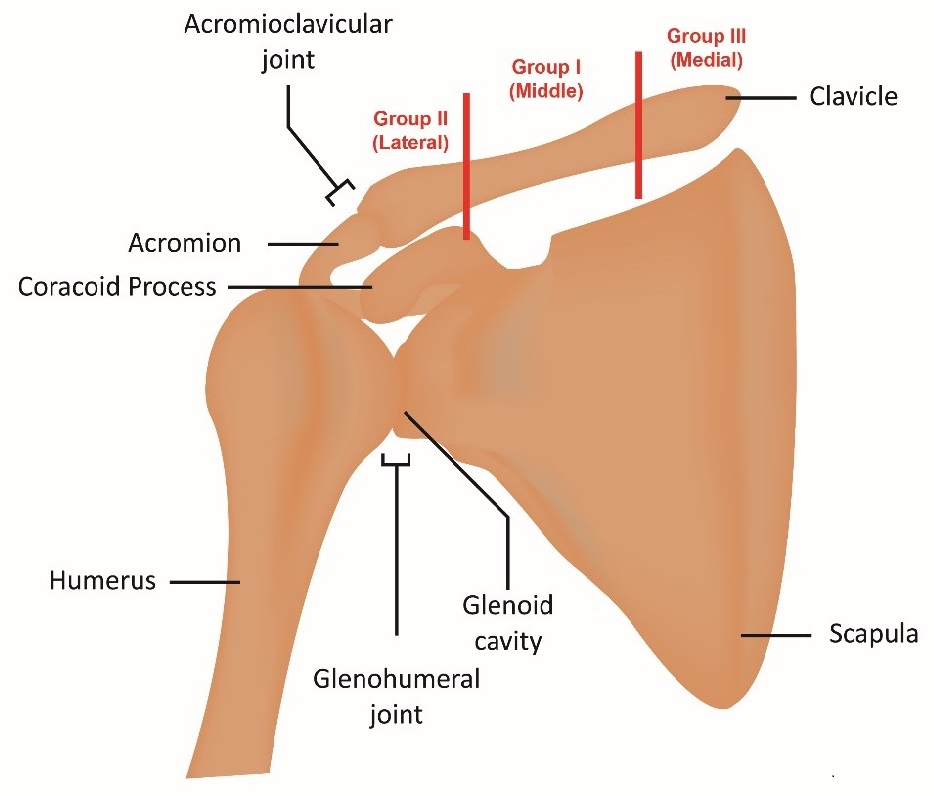
Classification based on anatomic location
Group I: Middle third (most common occurring 76-85%)
Group II: Distal third (10-21%)
Group III: Medial Third (3-5%)
Physical Examination
Patients typically present with moderate to severe pain in the shoulder, refusal to move arm on affected side, or swelling and bruising, along with a bony deformity.
Evaluation: Imaging
Anteroposterior radiograph is the standard study used. Other views used include cephalad-caudad (helpful to assess degree of displacement), apical-oblique (suited to identify fractures in the middle 1/3), apical-lordotic and axillary lateral view. CT may be useful for medial physeal fractures and sternoclavicular injuries.
Management
- Non-operative - Sling immobilization. The goal is to immobilize and prevent shortening of the clavicle on healing. A sling is used for nondisplaced middle and medial third fractures as well as stable distal/lateral fractures. There is s a small chance of nonunion especially with comminuted fractures and those with displacement results in shortening of >2cm. Sling immobilization may result in decreased shoulder strength and endurance even after healing.

- Operative – Open Reduction, Internal Fixation (ORIF)
ORIF method results in faster union, improved functional outcome, better cosmetic results, and improved over all shoulder recovery.
Possible complications include: hardware prominence (25-30%), neurovascular injury (3%), nonunion (1-5%), infection (4-5%), mechanical failure (1-2%) and adhesive capsulitis (4%).
|
Operative - Open Reduction, Internal Fixation (ORIF) |
||
|---|---|---|
|
ORIF method results in faster union, improved functional outcome, better cosmetic results, and improved over all shoulder recovery. |
Indication |
Relative Contraindication |
|
|
Nondisplaced fractures Skin intact Medically unfit for surgery |
Open fractures Multiple extremities injured Skin tenting or impending skin necrosis |
|
|
Comminuted fractures Fractures with 100% displacement fractures Prolonged nonunion Open fractures Floating shoulder Neurovascular involvement Significant shortening (>2 cm) Vertical fragment Infection |
Infection Severe skin condition (eg. acne) Stroke patient with little extremity usage |
| Indications for Operative and Nonoperative Management | ||
| Management
|
Indication
|
Relative Contraindication
|
|
Nonoperative
|
Nondisplaced fractures Skin intact Medically unfit for surgery
|
Open fractures Multiple extremities injured Skin tenting or impending skin necrosis
|
|
Operative
|
Comminuted fractures Fractures with 100% displacement fractures Prolonged nonunion Open fractures Floating shoulder Neurovascular involvement Significant shortening (>2 cm) Vertical fragment Infection
|
Infection Severe skin condition (eg. acne) Stroke patient with little extremity usage
|
QuickCheck
![]()

