Knee Injuries
Differential diagnoses may vary depending on the location of the knee pain.
| Anterior |
Posterior |
Lateral |
Medial |
|---|---|---|---|
|
|
|
|
Osgood-Schlatter Disease
(Osteochondrosis of the Knee or Tibial Tuberosity Apophysitis)
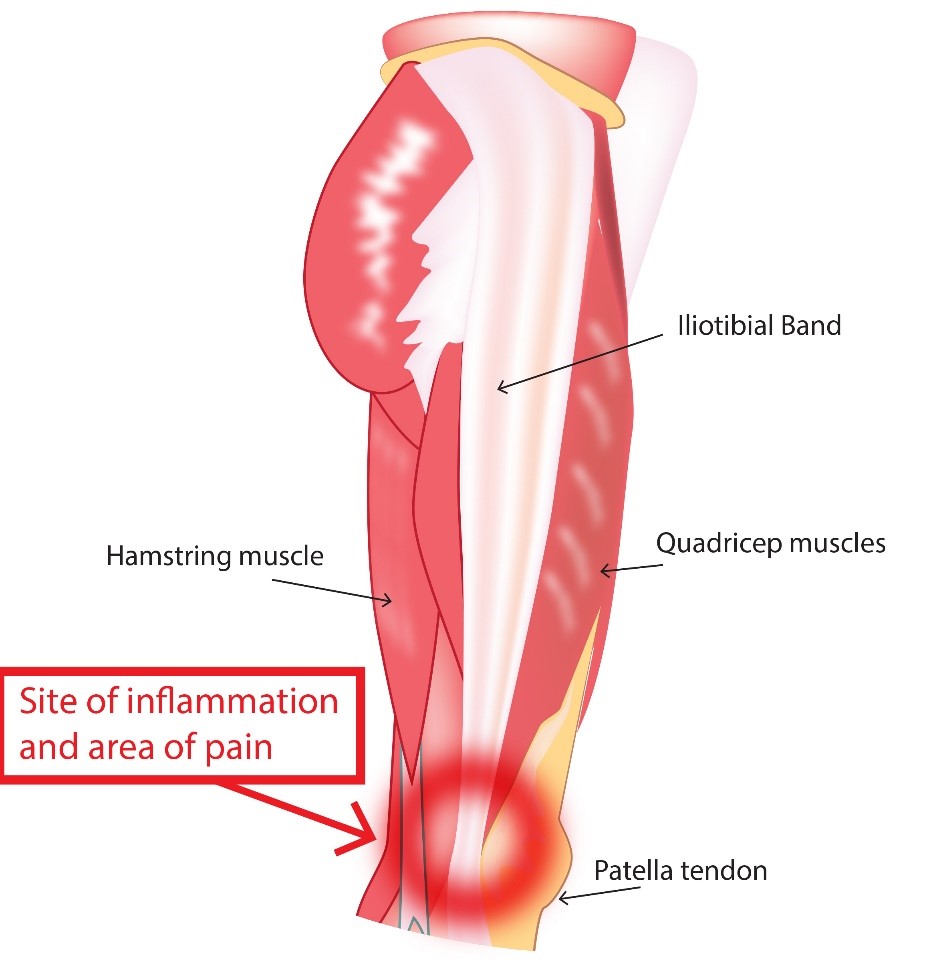
Osgood-Schlatter Disease is a common cause of chronic anterior knee pain in young athletes that presents with significant pain, tenderness and swelling at the insertion point of the patellar ligament on the tibial tubercle. The patellar ligament connects the quadriceps muscles to the superior pole of the patella and then the inferior pole of the patella to the proximal tibia at the tubercle.
Pain progressively worsens over time with continuous overuse eventually leading limitation of activity. Pain is aggravated by any direct trauma to knee, kneeling, squatting, climbing stairs or running and is relieved with rest and ice. Adolescents between the ages 9-14 who are experiencing a rapid growth phase and participating in activities or sports that involve running, jumping, cutting or squatting thereby increasing their risk for the development of OSD. Male prevalence but as female sports participation increases so has the incidence of OSD in females. Typically, unilateral knee affected (asymmetric) but bilateral in 25-50% of cases.

Note that the location of the pain distinguishes Osgood-Schlatter (pain in the tibial tuberosity) from Sinding-Larson-Johansson (pain in the inferior pole of the patella). Both conditions are due to microtrauma to the apophysis (growth plate that provides a point of attachment for the muscle and its associated tendon or ligament) in a skeletally immature but active child.
Mechanism of Injury
Exact cause is unknown but chronic repetitive trauma to the maturing proximal tibial growth plate by excessive force exerted on the secondary ossification center or apophysis by the patellar tendon leading to avulsion and tibial fragmentation with soft-tissue swelling of tubercle. The injury results in callous formation as healing occurs resulting in prominence of tubercle.
Physical Examination
Diagnosis is made by clinical exam. There is typically tenderness with soft-tissue swelling over the tibial tuberosity without erythema or warmth. Reproducible pain can be elicited with knee extension against applied resistance, during squatting with knee in fully-flexed, or with significant stress applied to quadriceps. Straight-leg raising usually is painless. Pain that is more prominent in the patellar tendon than the bony prominence is suggestive of patellar tendinopathy (jumper's knee).
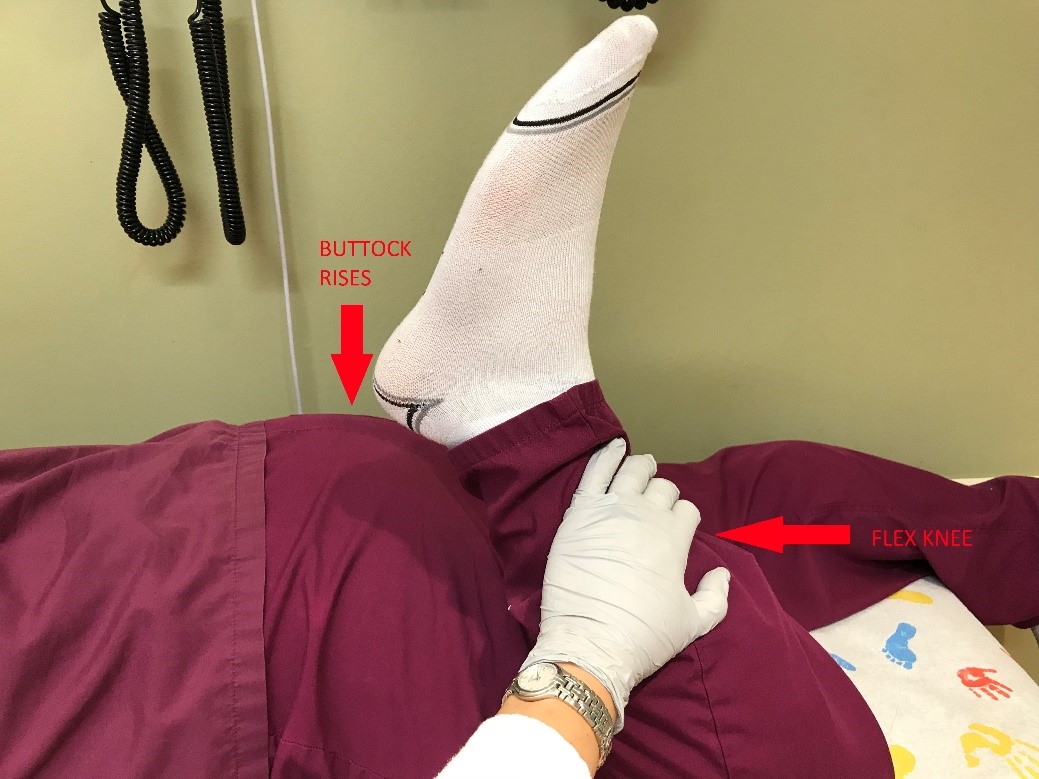
Ely Test
This test detects contracture of the rectus femoris component of the quadriceps muscle. With the patient prone, the examiner gently flexes the knee to 130 degrees. Contracture of the rectus femoris is indicated by simultaneous flexion of the hip, which causes the buttocks to rise off the table. Tight quadriceps or hamstrings have decreased elasticity or flexibility resulting in increased force on the patellar ligament.
Evaluation: Imaging
Lateral view may show soft-tissue swelling anterior to tibial tubercle. Other radiograph findings may include elevation or increased density of the tubercle, thickening or calcification of patellar ligament, or presence of bony fragment present within the patellar ligament, infrapatellar bursa edema.

Image source: http://www.radpod.org/2008/03/25/osgood-schlatter-disease/
Management
Osgood-Schlatter Disease is usually a benign and self-limiting disorder that resolves with closure of proximal tibial growth plate at 14-18 years. Tubercle prominence may be persist after growth plate closure, but pain and tenderness are no longer present.
Non-operative treatment involves "RICE" treatment for swelling reduction and analgesic medications for pain control. Limitation of activities that exacerbate symptoms is encouraged if pain does not resolve in 24 hours or pain is not tolerated. Using a brace or padding over the knee for protection and support of knee during activities (patellar tendon strap or taping between kneecap and tibial turbercle). Strengthening and stretching exercises or physical therapy can help increase flexibility of quadriceps and hamstrings. Patients with persistent pain greater than 3 months may benefit from injection of hyperosmolar dextrose (12.5%) mixed with lidocaine by the orthopedist.
Surgical intervention involves tibial tuberosity excision or ossicle resection in patients who fail conservative management. Surgery is usually not performed until the growth plates close.
Quadriceps & Patellar Tendinopathy
This is an overuse injury in jumping athletes. Upon presentation, they have pain localized to the superior border of the patella that worsens with activity. There is frequently associated swelling to the affected area also. Risk factors are sports that highly involve jumping (basketball, volleyball, long/high jump).
Mechanism of Injury
The injury occurs as a result of repetitive eccentric contractions ( motion of an active muscle while it is lengthening under load ) of the extensor mechanism. Microtears of the tendon most commonly at the bone-tendon interface then inflammation of the suprapatellar tendon of the quadriceps muscle.
Physical Examination
There is tenderness to deep palpation at quadriceps tendon insertion at the patella. A palpable gap over the affected area would suggest a quadriceps tendon tear. Upon evaluation the range of motion, there is pain upon knee extension but patient is able to actively extend the knee against gravity.
Evaluation: Imaging
- X-rays : Recommended views include AP and lateral. Optional view are sunrise or Mechant views for evaluation of patellar instability. Usually, radiograph findings are normal. Occasionally, there are tendon calcinosis are seen in chronic degeneration.
- Ultrasound is more effective at detecting and locating disruption in tendon.
- MRI is the most sensitive imaging modality. Common finding is the thickening of the affected tendon.
Management
Usually a non-operative approach is the mainstay of therapy: activity modification (rest until pain is improved), NSAIDs, and physical therapy. Cortisone injections are contraindicated due to risk of tendon rupture.
Prepatellar Bursitis (Superficial Infrapatellar Bursitis)
The prepatellar bursa is a potential space that functions to enhance gliding of tissue over the patella. This injury is caused by excessive kneeling. It is generally seen in wrestlers. Aseptic bursitis occurs more commonly, but septic bursitis can also occur.
Physical Examination
Localized tenderness and swelling is notable over the prepatellar region (anterior to the patella or patellar tendon) but it can also be warm to touch (especially if septic).
Evaluation: Imaging
X-rays (AP and lateral views) of the knee should be obtained in all patients with suspected acute bursitis. Knee ultrasound or MRI are usually not necessary for diagnosis. In chronic bursitis, CT, MRI, or bone scintigraphy may be helpful to determine if underlying osteomyelitis is present.
Bursal aspiration by the orthopedist is the key component of evaluation of knee bursitis to exclude septic bursitis.
Management
- Refer to the Orthopedic team to evaluate and potentially aspirate affected area.
- Non-operative: compressive wrap and NSAIDs. Use of corticosteroid is controversial.
- Operative: bursal resection is rare.
Iliotibial Band Tendinopathy (Iliotibial Band Syndrome)
Iliotibial Band Tendinopathy is a result of excessive friction between the iliotibial band (ITB) and lateral femoral condyle, subsequently causing ITB tensioning and inflammation. This injury is most commonly seen in runners, cyclists, and other athletes with repetitive knee flexion and extension.
 Symptoms
Symptoms
There is a localized pain over the lateral femoral condyle that is exacerbated with running. The pain is usually relieved with rest.
Physical Examination
Palpation over the lateral femoral condyle provokes localized pain. Range of motion of the affected leg elicits knee joint crepitus, reduced hip and/or knee range of motion due to pain, weakness upon hip abduction, and pain reproduced with single leg squat.
Ober test assesses the tightness of ITB. It is performed with the patient lying on the unaffected side. The examiner slightly abducts and extends the affected hip and flexes the knee. The patient is then asked to allow the affected leg to fall to the table passively, without actively adducting the hip (just letting it fall with gravity), while the examiner supports the patient's lower leg. Patients with ITB syndrome are more likely to have limited adduction of the leg with this maneuver (positive Ober test).
Image Source: https:https://www.bodyheal.com.au/blogs/sports-injuries/iliotibial-band-syndrome-symptoms-causes-treatment
Image Source: http://indianapolisfitnessandsportstraining.com/really-band-friction-syndrome-runners/
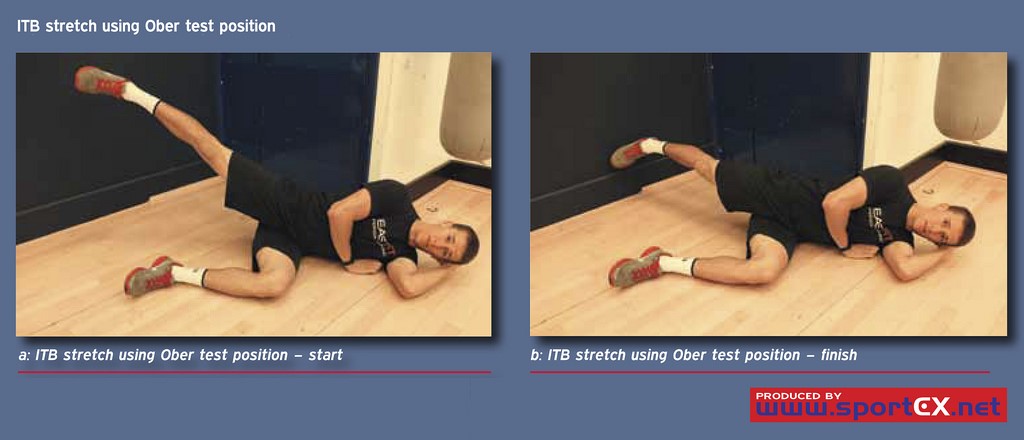
Image source: https://www.flickr.com/photos/sportex/8076561890
Evaluation: Imaging
- X-rays: AP and lateral views of the knee are the recommended views. Oblique and skyline views are additional views. Radiographic findings are usually normal. However, abnormal findings include medial joint compartment narrowing, patellar malalignment, and fractures.
- MRI: obtain if other soft-tissue pathology needs ruling out (ie. meniscal/ligamentous tears).
Management
- Non-operative: initial treatment is to reduce pain and swelling. Conservative measure include rest, ice, and NSAIDs. Corticosteroid injections may be considered if conservative measures fail. Physical therapy and training modifications are also beneficial.
- Operative: surgical excision
Meniscal Tear
Overview
The lateral and medial menisci are thickened cartilage that act as cushions between the tibial-femoral joint. Meniscal tears occur mostly in adolescents engaged in sports including soccer, basketball, and football that involve deceleration and a sudden change in direction with the knee partially flexed and the foot planted. The medial meniscus is more commonly injured than the lateral meniscus with injury occurring through a twisting or pivoting mechanism also involving compression with or without varus/valgus applied forces.
The meniscus in the adolescent is comprised of three parts or thirds:
- Outer part/third – appears red as it is well-perfused by generous blood supply from the synovium
- Middle part/third – appears red-white as it has some blood supply to its outer margin
- Inner part/third – appears white as it is avascular or without blood supply
Tears are classified as longitudinal or radial based on the meniscal surface and as complete or incomplete according to the depth of the tear.
- Longitudinal tear – when displaced, it appears like a "bucket-handle" and are the most common type of tear in the young athlete.
- Radial tears – begins in the inner third or avascular region
A meniscal tear may present initially with pain followed by swelling over a 24 hours period and/or pain aggravated by pivoting motions of the knee. A "tearing" or "popping" sensation may also be felt at the time of injury. Mechanical symptoms such as "catching" or "locking" coupled with a feeling of instability or the knee "giving out" may also be reported. The sensation of "locking" or "catching" is created by a portion of the torn meniscus interfering with the ability to fully extend the knee as the fragment interposes between the articular surfaces of the femur and tibia. Altered proprioception caused by the detached meniscal fragment moving around between the articular surfaces also results in perception of instability
Physical Examination
The type and location of the meniscal tear influence the accuracy of the physical exam with partial, horizontal, or anterior tears often resulting in a normal knee exam as these tears do not impede the normal knee mechanics. Patients with meniscal tears may present with lateral knee pain with tenderness to lateral joint line and decreased range of motion that may inhibit full extension of the knee. A joint effusion may also be present in larger or more complex meniscal tears. Effusions may reduce knee flexion and may be reported as joint stiffness.
Three tests can be used to produce the catching or locking sensation that is associated with meniscal tears.
Thessaly Test
Attempts to recreate the loading forces applied to the knee. The clinician and patient face each other while standing and hold hands for support. The patient stands on one leg with knee flexed around 20 degrees. The patient then rotates their knee and body while maintaining knee flexion which rotates the knee both internally and externally while putting force on the meniscus. Perform the test on the unaffected side first for comparison and so the patient can learn the maneuver then test the affected side. Eliciting pain or reproducing the catching/locking sensation constitutes a positive test.
McMurray Test
Involves repeated passive knee flexion and extension to assess for joint motion tenderness and to detect meniscal injury. The patient is supine with the clinician holding the patient's heel with one hand and placing the other hand along the joint line. The knee is passively flexed to as near 90 degrees as possible as the examiner rotates the tibia internally while gradually extending the knee. Repeat passive full flexion and extension of the knee with tibia in internal rotation is then followed by passive flexion of the knee with external rotation of the tibia which is repeated several times. Varus and valgus pressure are sometimes applied during passive flexion and extension to increase stress on meniscus as may help detect injury. A painful snap or click in early- or mid-extension that may be sometimes felt or heard or pain elicited along the joint line with maneuver are suggestive of meniscal tear. This maneuver tests the posterior and middle portions of the meniscus and therefore anterior or anterolateral tears may not be detected reliably with this test. Thus, a negative test does not completely rule-out a meniscal tear.
Apley Compression Test
The patient in prone position with affected knee flexed 90 degrees while the examiner their own hand or knee to stabilize the patient's thigh. The clinician then moves the patient's heel toward the floor or exam table while rotating the foot internally and externally and the knee is extended. This maneuver results in the compression of the meniscus between the tibial plateau and the femoral condyles. Eliciting pain with compression of meniscus results in a positive test.
Evaluation: Imaging
- X-rays include postero-anterior, weight-bearing anteroposterior, lateral, sunrise, and tunnel/notch views may be appropriate, especially if patient has tenderness over proximal fibula or patella, decreased knee flexion or cannot bear weight. The notch view may reveal a loose body or osteochondral defect.
- Ultrasound may be used to compare knee dynamics of affected knee with unaffected knee. It cannot be used to assess the deeper internal structure of the knee.
- MRI is a preferred modality for determination of the degree of injury and the type of meniscal injury, but is often only employed in cases where surgery is a consideration. MRI is required in patient with presence of frequent mechanical symptoms or persistent effusion or if symptoms persist for 3-4 weeks of medical management. MRI can detect both medial and lateral meniscal tears but with varying sensitivity and specificity.
Evaluation: Other
- Joint aspiration may be required in cases with rapid development of a large effusion (within 2-3 hours of injury) to exclude hemarthrosis or bleeding in the joint which is seen in meniscal tears with associated ACL tears. Fat globules present in aspirate usually indicate a fracture.
Management
Management depends on the type of tear and on the presence of instability, mechanical symptoms, persistent effusion or hemarthrosis. Small tears that are rarely symptomatic and do not interfere with normal knee mechanics and function can be managed conservatively.
Conservative measures: Rest the knee. Avoid maneuvers or activities that apply pressure on the knee joint until swelling subsides including squatting, kneeling, pivoting, or movements that require repetitive flexion/extension of knee joint like climbing stairs. Apply ice to the knee for 15-20 minutes every 4-6 hours with leg elevated may help reduce pain and swelling. Use crutches to reduce weight-bearing on affected knee. Utilize a knee brace that restrains patellar motion to prevent knee "giving out." Pain management, as needed. Conservative management is likely to be successful in cases where symptoms develop more slowly over 24-48 hours (rather than immediately), minimal swelling is present, full range of motion of the knee with pain is present only during full flexion or nearly full flexion of knee, or McMurray Test elicits pain only during deep flexion.
Physical therapy
- Straight-leg raising exercises can help to develop and strengthen quadriceps with light weights added to ankle as quadriceps strength improves.
- Walking, water aerobics or swimming may also help strengthen muscles that support the knee.
- Exercises requiring deep knee flexion should be avoided until pain and swelling subside.
Orthopedic referral should be made for determining type of tear and degree of tear and whether surgical intervention is necessary. Immediate orthopedic referral should be made for large complex tears with persistent effusion, tears resulting in frequent mechanical symptoms, or "locking" of knee with extension as surgical intervention is likely necessary.
Arthroscopic or open knee surgery with partial meniscectomy is preferred over total meniscectomy as it results in less recovery time and it reduces risk of developing of osteoarthritis. Osteochondritis dissecans of the lateral femoral condyle is a rare complication following partial and total meniscectomy secondary to repetitive compression of the immature chondral structures.
Surgical Intervention is likely to be required when the following factors are present:
- Severe twisting of knee and unable to resume activity following injury
- Limited range of motion or knee is in a "locked" position
- McMurray Test elicits pain with minimal flexion of knee
- Associated ACL tear
- Minimal improvement in symptoms after six weeks of appropriate conservative management
Discoid Meniscus
Overview
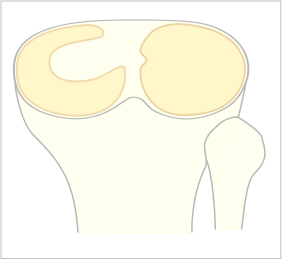
Discoid Meniscus is a term that describes an anatomic abnormality of the shape of the meniscus that results in a larger, thicker meniscus that resembles a "disc" rather than the normal "crescent" shape. It typically involves the lateral meniscus but can be bilateral in a small percentage of affected individuals.
A specific cause for developing a discoid meniscus is unknown but may be a congenital anomaly or due to other contributing genetic and familial factors. Discoid menisci demonstrate a "disorganized collagen fiber scaffold" formation which increases the incidence of meniscal tears with horizontal tears being the most common.
Patients with this abnormally-shaped meniscus may be asymptomatic especially in early childhood as the menisci are stable and no tearing has occurred. Older children and adolescents may present with chronic pain, an intermittent history of knee popping or clicking, effusion, quadriceps atrophy, limited ROM, as well as other mechanical symptoms such as locking or "giving way".
Classification of discoid menisci is based meniscus shape and its stability based on the degree of hypermobility and peripheral rim detachment. Unstable incomplete or complete menisci can be further differentiated by location of instability (anterior, middle or posterior horn).
Image source from Wikimedia Commons: https://commons.wikimedia.org/wiki/File:Scheibenmeniscus.svg
- Complete Type - disc-shaped meniscus covers the entire lateral tibial articular surface or plateau with normal posterior attachment
- Incomplete Type - semilunar meniscus that covers < 80% of lateral tibial articular or plateau with normal posterior attachment
- Wrisberg Type - more crescent-shaped or normally shaped than other types but lacks the normal posterior meniscal attachments including the coronary ligament. Only the Wrisberg ligament is connected to the posterior horn of the lateral meniscus resulting in hypermobility of the lateral meniscus and meniscal shift with knee flexion and extension leading to "snapping" or a "clunk" heard at the end of flexion.
Physical Examination
Tenderness along the joint line, effusion, and meniscus may be felt when laterally snapping out of joint. An unstable discoid meniscus secondary to peripheral rim detachment may result in the meniscus moving into the intercondylar fossa when the knee is extended resulting in a snapping sensation, audible crepitus, and a swelling or bulge noted to the anterior joint line. A "clunk" also may be felt or heard at end of flexion. The McMurray Test as discussed above may be used to detect a discoid meniscal tear.
Evaluation: Imaging
- X-rays may show widening of lateral joint space, elevation of fibular head, and lateral femoral condyles may appear "squared" suggestive of presence of rectangular tissue (discoid) which flattens the edges of the condyles.
- MRI without contrast is the preferred imaging modality for diagnosis of discoid meniscus which often appears as an abnormal, thickened "bow-tie" shape. MRI can detect tears and meniscal shift but is not useful in determining the degree of stability. Some incomplete discoid menisci may also be missed as the can appear normal MRI.

Source: images.radiopaedia.org
- Diagnostic arthroscopy may be necessary to confirm diagnosis in symptomatic individuals with normal MRI findings.
Management
Asymptomatic discoid menisci do not require treatment even when snapping is present. However, management includes observation if found incidentally during another study as discoid menisci are vulnerable to tears.
Discoid menisci that are symptomatic generally require surgical intervention with partial meniscectomy being more common than total meniscectomy to reduce risk of osteoarthritis that often results when the entire meniscus is removed. Arthroscopic partial meniscectomy or "saucerization" involves the removal of central portion of meniscus with preservation of the stable peripheral rim with or without repair of peripheral rim detachments. This procedure effectively reshapes from disc into crescent-shape which is more anatomically correct but the remaining portion of the discoid meniscus is still prone to tears.
Ligamentous Injury
Knee Ligament Anatomy
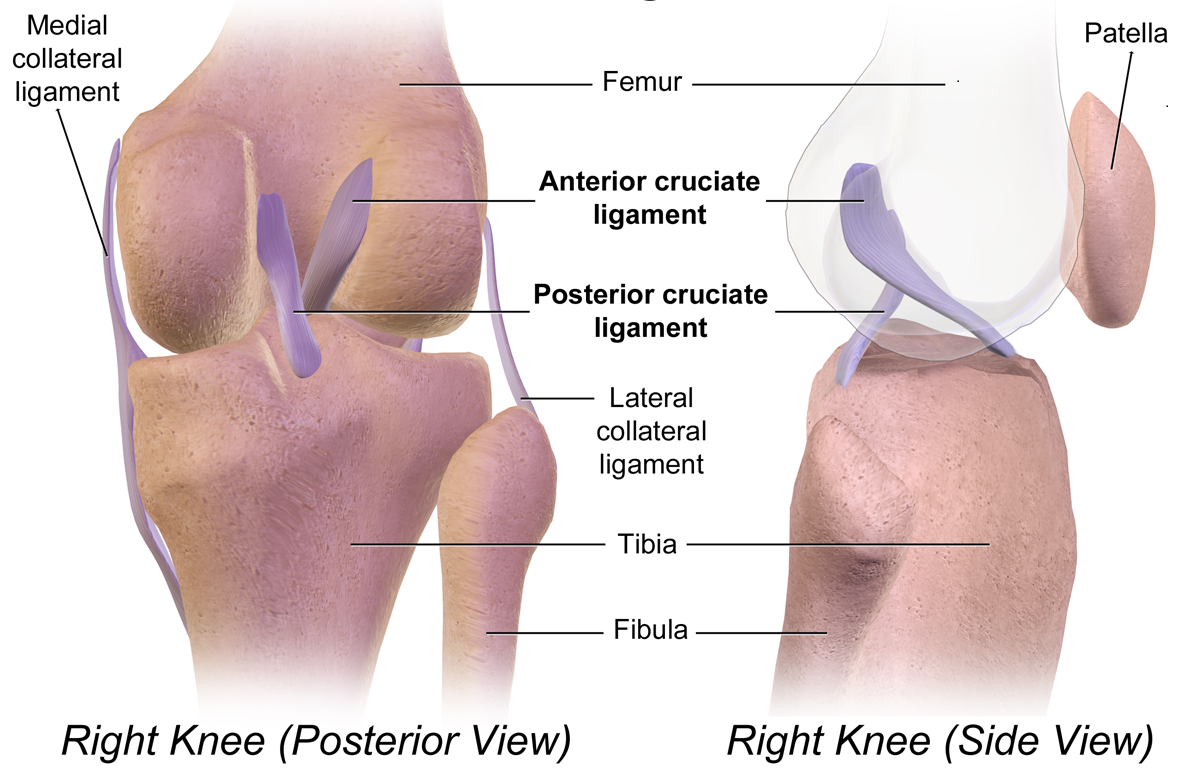
Image Source from Wikimedia Commons: https://commons.wikimedia.org/wiki/File:Cruciate_Ligaments.png
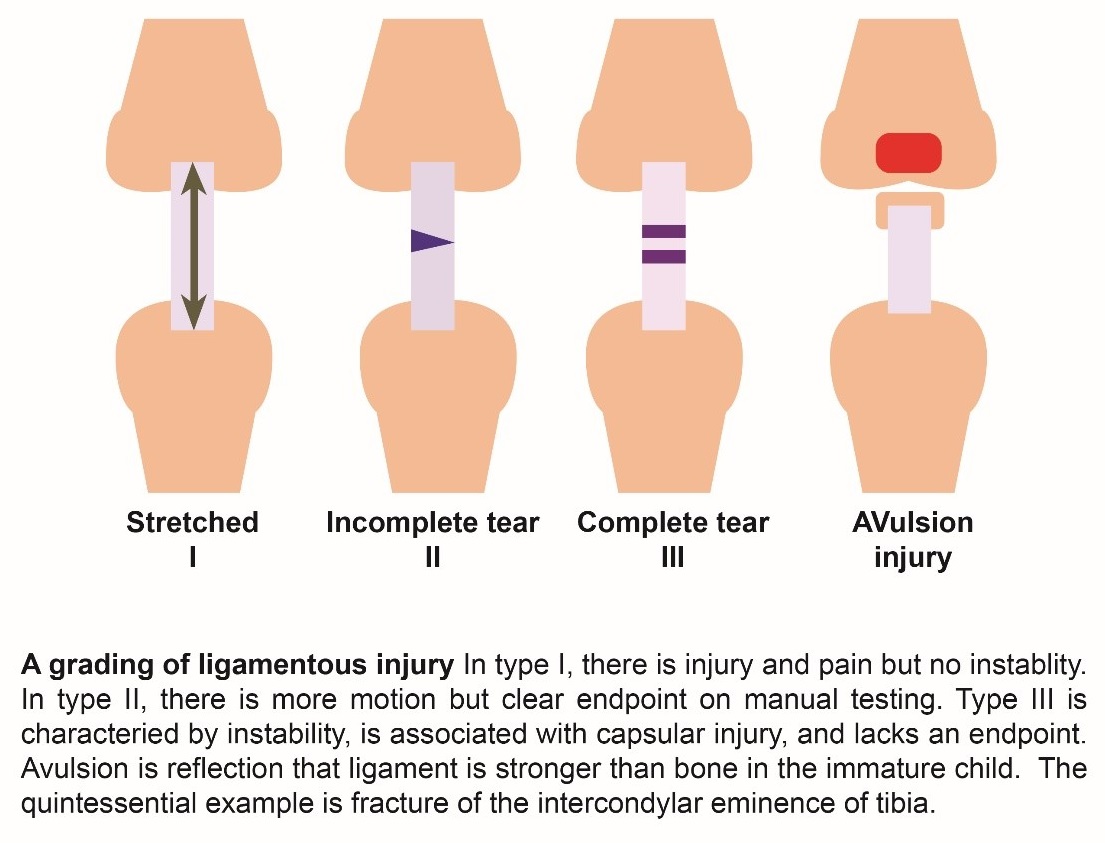
Grading of Ligamentous Injury
ACL: Anterior Cruciate Ligament
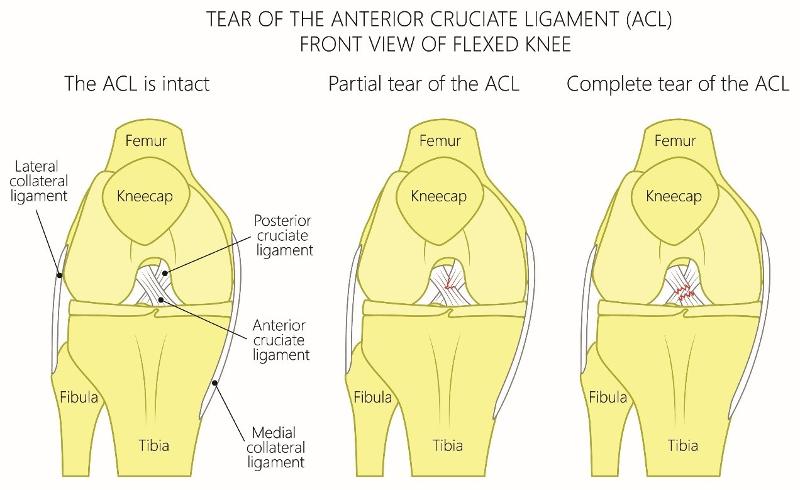
ACL tears are a common injury in adolescents participating in sports that involves running and cutting such as volleyball, soccer, basketball, skiing and football. Most common mechanism typically involves a low-energy noncontact injury that involves sudden deceleration or sudden stop combined with a twisting or pivoting motion that increased valgus stress or lateral bending of the knee.
A non-contact injury can occur when running and then suddenly changing direction in effect twisting the knee or via contact injury when the foot is planted on ground and a subsequent valgus force is applied to the knee during a collision (common in football); or the athlete falls in a way that results in rotation or lateral bending of the knee. ACL injury can also be secondary to high-impact force such as in a motor vehicle collision with direct force applied to the lateral knee.
Female athletes are more likely than males to sustain ACL injury due to differences in muscle strength and development, poor biomechanics, and the effects of estrogen on ligament laxity, strength, and flexibility.
Patients typically present with lateral knee pain, effusion, decreased ROM, and inability to bear weight immediately after injury. Patients may report a "popping" sensation at time of injury. Pain and swelling gradually subside over after several weeks as does the ability to bear weight. However patients often report instability of the knee with episodes of knee "giving out" or "giving away" when performing pivoting or cutting motions.
Physical Examination
ACL on physical exam usually involves the Anterior Drawer, Lachman, and Pivot Shift tests which can detect increased forward motion of the affected knee albeit these test have less sensitivity if performed immediately after injury due to presence of pain and swelling.
- Anterior Drawer Test: This test is performed with patient supine with hips flexed and knees in 90 degree flexion and feet flat on exam table. The proximal tibia is grasped with both hands with thumbs placed on the lateral and medial joint line and fingers on the medial and lateral insertion points of the hamstrings. Gently pull the knee forward and observe for increased anterior forward motion as compared to opposite knee. Increased anterior or forward movement is regarded as a positive test.
- Lachman Maneuver: This test is more sensitive than the anterior drawer test. The patient is supine with knee flexion between 15 and 30 degrees with slight external rotation of the hip and knee; the proximal tibia is pulled forward and moving the distal femur back with the opposite hand. Increased anterior or forward movement constitutes a positive test.
- Pivot Shift Test: It is highly specific for ACL injury but may be difficult to perform due to guarding and is only sensitive if patient is relaxed during maneuver. Patient is supine and knee is initially in extension, the lower leg is held in one hand while internally rotating the tibia as valgus stress in placed on the knee with the other hand which causes subluxation of the tibia. While maintaining these forces, the knee is flexed with this maneuver resulting in reduction of the subluxed of the tibia in the ACL-deficient knee and is felt as a "clunk" by the clinician and is considered a positive test.
Evaluation: Imaging
Diagnosis can be made with physical exam findings but imaging can support clinical diagnosis.
- X-rays often demonstrate normal findings but should be obtained with anterior-posterior, lateral, notch views to assess for fractures including avulsion fracture of anterolateral tibial plateau known as Segond's fracture which often correlates or suggests underlying ACL or meniscal injury.

- MRI is usually obtained to support diagnosis as it is both highly sensitive and specific in identifying and diagnosing ACL ruptures.
|
|
|
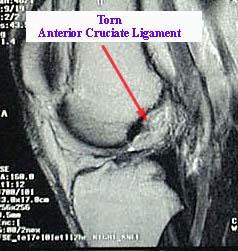
Source: emedx.com
- Knee arthroscopy is the gold standard in ACL diagnosis.
Management
In the acute setting, patients with history and findings suggestive of ACL injury should be placed in a knee brace and given crutches to avoid weight-bearing protecting against further injury. Elective outpatient referral to orthopedic surgeon should be placed with evaluation made within 7-14 days post-injury.
Non-operative treatment is an option for those that do not plan to return to sports activities and includes physical therapy with quadriceps strengthening and neuromuscular rehabilitation.
Surgical reconstruction is usually required for those desiring to return to sports activities as recurrent knee instability may interfere with ability to play sports that involve pivoting motion.
PCL: Posterior Cruciate Ligament
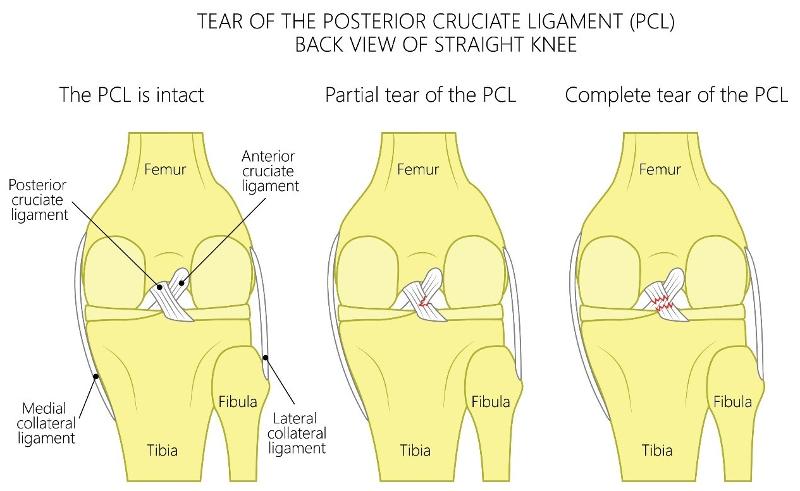
PCL injuries are less common than ACL injuries in athletic activities with injury occurring secondary to a fall with knee in flexion and foot in plantarflexion or due to a direct blow or posterior sheer force applied to the anterior knee. The PCL and the posterior capsule may also be injured with hyperextension or hyperflexion of the knee with or without a direct posterior force. PCL injury can also occur in motor vehicle accidents when a posteriorly directed force is applied to a knee in a fixed position and often due to a dashboard hitting the flexed knee.
Patient may present with knee instability especially if the injury also involves other posterolateral knee structures. However, isolated PCL injuries albeit rare may be more difficult to detect when other structures not involved. A "pop" may not have been felt at time of injury as opposed to ACL injury. Patient may have mild-to-moderate effusion and a limp noted during ambulation suggesting pain with weight-bearing. Patients may also report posterior knee pain especially when kneeling down or squatting and may demonstrate loss of terminal knee flexion and unable to bend knee the last 10-20 degrees. Patient may describe generalized knee pain or that something is wrong with their knee but unable to be more specific.
Isolated PCL injuries can be classified as acute or chronic. Acute injuries often present with antalgic gait as well as other gait abnormal gait patterns depending on extent of injury and patient's specific anatomy.
Physical Examination
- Posterior Drawer Test: Performed with patient supine with hips flexed and knees in 90 degree flexion and feet flat on exam table. The proximal tibia is grasped with both hands with thumbs placed on the lateral and medial joint line and fingers on the medial and lateral insertion points of the hamstrings. Gently push the knee backward and observe for increased posterior backward motion in the femur as compared to opposite knee.
Grades of PCL injury are based on Posterior Drawer Test:
Grade 1 (0-5 mm posterior displacement) – anterior border of medial tibial plateau can be posteriorly displaced but still remains anterior in relation to medial femoral condyle; few fibers are torn.
Grade 2 (6-10 mm posterior displacement) – anterior border of medial tibial plateau can be posteriorly displaced but is even with the medial femoral condyle.
Grade 3 (>10 mm posterior displacement) – anterior border of medial tibial plateau can be posteriorly displaced past the medial femoral condyle.
- Posterior Sag Sign (Godfrey Test): when a PCL injury is present, the tibia "sags" when compared to the unaffected knee.
- Quadriceps Active Test: when the quadriceps are contracted, the tibia moves forward or anteriorly from its posterior subluxed position.
Evaluation: Imaging
Diagnosis can be made with physical exam findings but imaging can support clinical diagnosis.
- X-rays often demonstrate normal findings but should be obtained with anterior-posterior, lateral, notch views to assess for fractures including avulsion fracture of anterolateral tibial plateau known as Segond's fracture which often correlates or suggests underlying ACL or meniscal injury.
- MRI is usually obtained to support diagnosis as it is both highly sensitive and specific in identifying and diagnosing ACL ruptures.
|
|
|
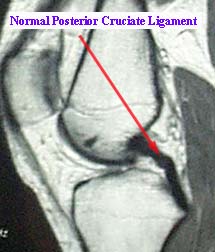
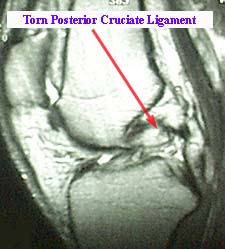
Image source: emedx.com
- Knee arthroscopy is the gold standard in ACL diagnosis.
Management
In acute setting, patients with history and findings suggestive of ACL injury should be placed in a knee brace and given crutches to reduce weight-bearing and to protect against further injury.
Elective outpatient referral to orthopedic surgeon should be placed with evaluation made within 7-14 days post-injury.
Non-operative treatment is an option for those that do not plan to return to sports activities and includes physical therapy with quadriceps strengthening and neuromuscular rehabilitation. For those desiring to return to sports activities, surgical reconstruction is usually required.
MCL: Medial Collateral Ligament
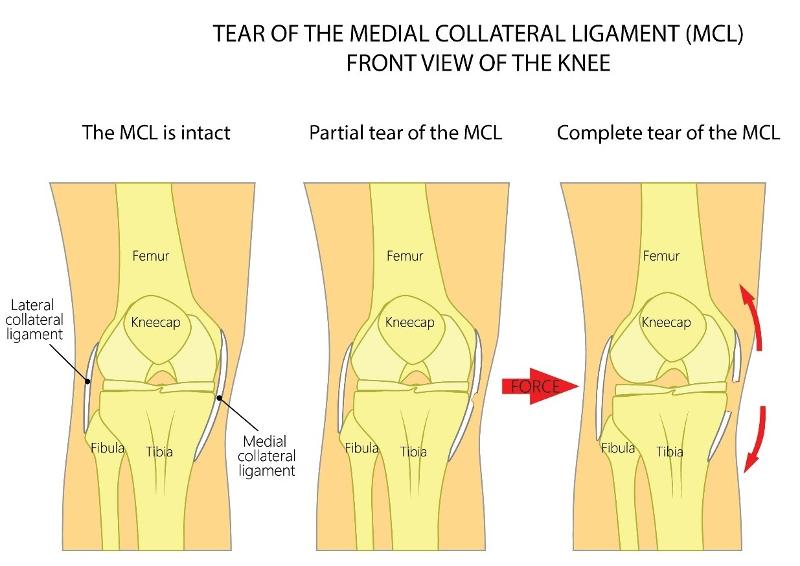
MCL tears occur when a valgus stress is applied to the lateral side of the knee suddenly forcing the knee medially into a "knocked knee" position. MCL injuries are more likely to involve other knee structures and associated meniscal tears.
Patients typically present with medial knee pain following a direct contact or collision with a valgus force applied to lateral knee while the foot is planted. Noncontact MCL injury may occur due to an abrupt valgus movement the results in the "knocked knee" deformation or knee bending medially while the knee is hyperextended with some external tibial rotation. Often occurs when an athlete catches their shoe, cleat, ski, or skate on a surface as they are quickly changing direction. Patients frequently report a sensation of knee instability especially during standing or walking. Swelling and mechanical symptoms such as locking and the knee "giving out" may also be present.
Physical Examination
The most common finding on exam is medial knee tenderness and localized soft tissue swelling. Valgus stress may reveal a widening of the knee joint.
Grades of MCL Tears
|
Grade 1 (0-5 mm of medial knee opening) - Mild tear or sprain of the ligament with some localized tenderness but no laxity or mechanical symptoms as only a few fibers are involved. Grade 2 (6-10 mm of medial knee opening) - Partial or moderate tear of the ligament with presence of localized or diffuse tenderness along the lateral or posterolateral knee. Some swelling and mild-to-moderate laxity are present but a solid endpoint is preserved indicating some ligamentous integrity is still intact. Grade 3 (> 10 mm of medial knee opening) - Complete tear of ligament with variable amount of pain. Laxity without a solid endpoint that results in mechanical symptoms and frequently associated with injury of other ligaments. |
Abduction Stress Test (also known as Valgus Stress Testing)
This is the most appropriate test for determining the extent of MCL injury. The clinician positions themselves such that one hand is placed on the lateral side of the knee to stabilize femur and the other hand is placed around the medial ankle. The clinician then pushes the knee medially while pulling the ankle laterally which opens the knee joint on the medial side. This maneuver is performed with the knee at both full extension and 30 degrees of flexion. Pain or a gap noted to the medial joint line at approximately 30 degrees indicates of ligamentous laxity and a partial tear of the MCL. Laxity at 0 degrees of flexion suggests possible injury to ACL, PCL, posteriomedial corner, and/or posterior oblique ligament.
Evaluation: Imaging
Minor injury of the MCL does not require imaging as damage is not usually seen on plain radiographs.
- X-rays : In the presence of bony tenderness of the medial femur, patella, fibula, or tibia in a suspected MCL (or LCL) tear then anteroposterior, patellar, and lateral x-ray views should be obtained. Valgus stress views may also be useful in identifying medial soft tissue injury and valgus instability in cases where MRI and ultrasound are not used.
- Ultrasound: Trained sonographers are able to use ultrasound to detect grade 1 or 2 injury with the MCL (or LCL) appearing hyperechoic and thickened. Grade 3 injuries also demonstrate hyperechoic thickening with disruption of fiber continuity, associated edema and hemorrhage, and increased laxity of the medial (or lateral in LCL) joint line.
- MRI: This is the most appropriate modality for assessing MCL (and LCL) injuries with both high sensitivity and specificity.
|
|
|
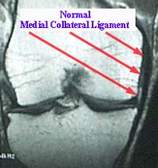
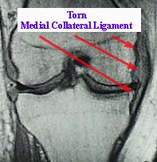
Image source: emedx.com
Management
Initial management of MCL injury is conservative management with rest, ice, immobilization and pain management as discussed in more detail under meniscal injuries. LCL injuries are managed similarly to MCL injury (see above)
Management is determined by grade of injury
Grade 1 - Crutches for up to 1 weeks and a hinged-brace worn for 4-5 weeks for all weight-bearing as it stabilizes medial and lateral knee but allows for flexion and extension of knee.
Grade 2 - Crutches and knee immobilizer for 1-3 weeks to reduce pain followed by gradual partial weight-bearing starting in week 2 or 3. Hinged-brace can be employed once partial weight bearing is achieved.
Grade 3 - Crutches and immobilization and non-weight bearing. Orthopedic referral as surgical intervention is usually required and performed two weeks post-injury.
LCL: Lateral Collateral Ligament
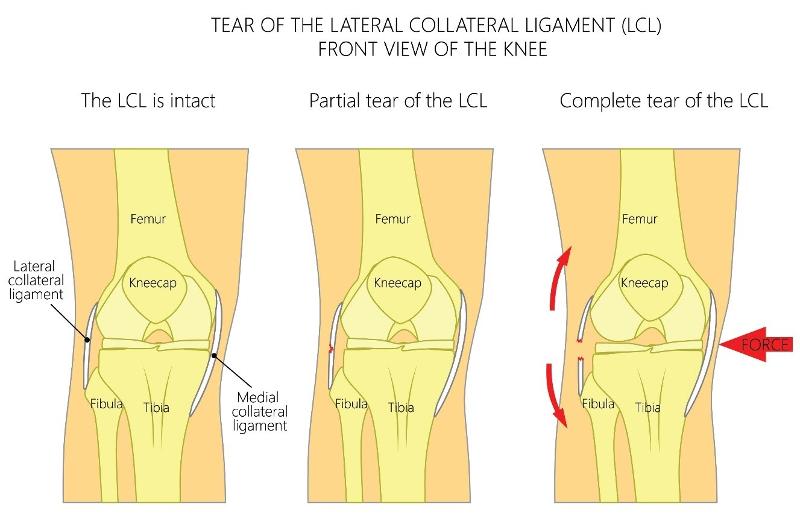
Isolated LCL injuries are the second least common knee injuries with isolated PCL tears being the least common. Isolated LCL tears occur when a varus stress is applied to the inside or medial side of the knee forcing the knee laterally LCL injuries are more likely to occur secondary to a high-energy impact injury that involves multiple knee structures such as the posterolateral corner of the knee, the lateral meniscus, the posterior cruciate ligament (PCL) and/or the anterior cruciate ligament.
Patients typically present with lateral or posterolateral knee pain after sustaining a direct hit or contact to the medial or anteromedial portion of the knee while the knee is fully extended. This often occurs in football when a player is being tackled and a posterior varus force is applied to medial knee while the foot is planted and the knee hyperextended.
Noncontact LCL injury may occur due to an abrupt varus movement results in the knee bending laterally while the knee is hyperextended. Therefore, a varus stress combined with some degree of hyperextension and/or external tibial rotation results in LCL injury.
Patients frequently report a sensation of knee instability especially during standing or walking. Swelling and mechanical symptoms such as locking and the knee giving out may also be present.
Physical Examination
- Arcuate sign: A small avulsion fracture of the styloid of the roximal fibula. This is specifically characteristic of a posteriolateral corner injury with a possible a distal LCL tear.
- Segond fracture (as discussed under ACL section) can also indicate LCL injury. Segond fractures result when a varus force results in the oblique attachment of the LCL to pull off a fragment from the tibial plateau.
Evaluation: Imaging
- X-rays, like minor MCL injuries, LCL does not usually require x-rays unless bony tenderness is present. Varus stress views on an x-ray may be useful in identifying lateral soft tissue injury and varus instability in cases where MRI and ultrasound are not used.
- Ultrasound findings are similar for LCL except laxity is noted at lateral joint line.
- MRI is the most appropriate modality for assessing LCL tears.
Management
Management of LCL tears is similar to MCL tears (see above).
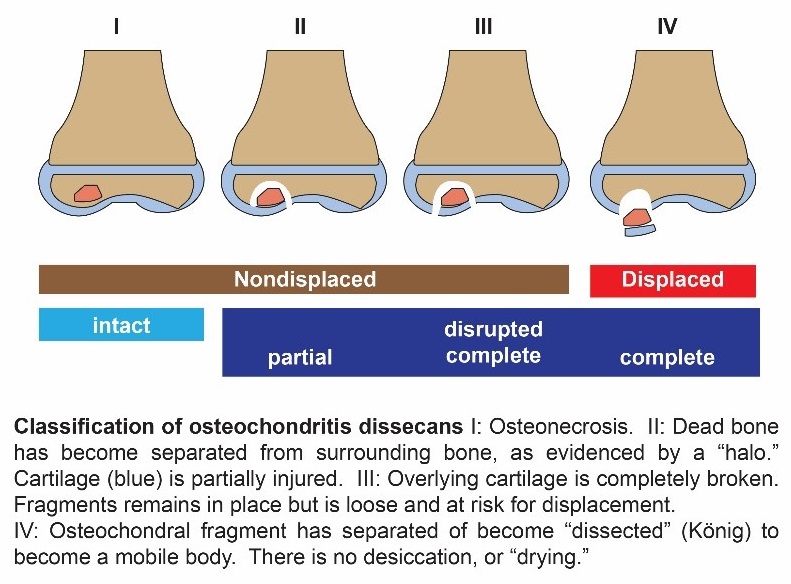
Osteochondritis Dissecans (OCD)
Osteochondritis Dissecans is called Juvenile OCD in skeletally immature patients or patients with open growth plates or physes.
OCD involves a lesion where a localized portion of subchondral bone and its corresponding articular cartilage become detached from the underlying bone resulting in ischemia and bone death. OCD may occur in knee, ankle, or elbow.
The ischemic bone fragment is considered stable if it remains in its original position but is classified as unstable if the fragment becomes displaced and is moving freely around the joint. Occurs most often in rapidly growing active school-aged children and adolescents. Males are more likely than females to develop OCD by a ratio of 2:1. Most common region for an OCD lesion is the lateral part of the medial femoral condyle (bilateral in 25% of cases).
Patient presents with knee pain and swelling with mechanical symptoms that can include catching or locking, sensation of knee instability or knee "giving out" as a displaced bone fragment interferes with normal range of motion
Mechanism of Injury
OCD involves a combination of traumatic injury to the knee with resulting ischemia and necrosis (death) of a segment of subchondral bone and its adjacent trabecular or spongy bone. The overlying articular cartilage attached to this area of necrotic bone remains viable as it receives it blood supply and nutrients from the synovial fluid. The necrotic portion of bone is gradually reabsorbed and is progressively replaced by new viable bone. A new trauma to the same area can result in disruption of the cartilage with dislodgment of the bone fragment leading to a loose or unattached body floating within the knee joint.
Physical Examination
Patients usually complain of non-specific, progressively worsening knee pain aggravated by activity or exercise. Development of intermittent swelling, crepitus, and joint stiffness during and after activity typically occur. Often, there is a sensation a mobile body or fragment in the joint interfering with mechanical function with catching or locking of knee or a feeling of instability with knee "giving out" and may develop an antalgic gait with lateral rotation of the foot on affected side to reduce pain with weight-bearing. Full range of motion is usually retained but tenderness when direct pressure is applied over the medial femoral condyle with the knee in full-flexion is indicative of OCD.
Wilson Sign: test used to diagnose OCD lesions of the lateral portion of the medial femoral condyle. The patient sits with the knee flexed over the exam table. The examiner actively extends the knee while medially rotating the tibia which elicits increasing pain as extension continues (or when knee reaches about 30 degrees of flexion). The maneuver is halted at this point and when the tibia is laterally rotated and the pain completely subsides.
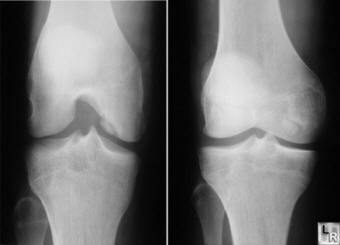
Evaluation: Imaging
OCD lesions can be classified based on imaging findings (plain radiograph, MRI, or arthroscopy).
- X-rays: should be first be obtained if the clinician suspects OCD to assess affected joint, including anteroposterior, lateral, notch or tunnel and sunrise views. Medial condylar OCD lesions are usually seen best with a lateral "notch" view. This view employs a 45-degree lateral "notch" or tunnel view which reveals a radiolucent crescent-shaped area of sclerosis that appears as a "halo".
- MRI: is often used when OCD is suspected but plain radiographs appear normal. MRI without contrast is sufficient for diagnosing and staging OCD lesions but gadolinium contrast is used to assess blood supply to bony fragment when stability is in question. MRI allows for visualization of loose cartilage and subchondral bone that is not detected by plain films. In skeletally immature patients, MRI requires clinical correlation and is not entirely reliable study for determining necessity for surgical intervention or stability of bone fragment.

Image source: learning radiology.com
- CT, ultrasound, and radionuclide bone scans: have also been used in diagnosis of OCD but plain radiography and MRI are usually adequate to make the diagnosis.
Management
Treatment is determined by OCD severity or classification according to Berndt and Hardy:
Stage I – Small compressed, non-displaced bone fragment
Stage II – Partially detached bone fragment
Stage III – Completely detached, non-displaced bone fragment
Stage IV – Completely detached, displaced bone fragment
Non-Surgical Interventions. Conservative management is usually adequate for stage I - III OCD lesions. Non-displaced fragments can be treated non-operatively through conservative measures that include NSAIDs/analgesics and no sports participation with resumption of activities only after symptoms completely resolve or imaging demonstrates complete healing of lesion. Immobilization with casting or hinged braces with limited weight-bearing for 6-12 weeks dependent on duration of healing. Physical Therapy for strengthening and increasing joint mobility after evidence of healing and weight-bearing with ambulation; swimming and cycling are often used for rehabilitation as these activities as they build muscle strength with low impact on joint.
Surgical Intervention. Indications for surgical intervention include:
Stage IV lesions which indicates a detached and displaced bony fragment
Lesion that have not responded to non-surgical treatment after 4-6 months
Lesions > 400 mm in size
Arthroscopy or arthrotomy can be uses to remove displaced fragments if non-weight bearing surface is not involved. Surgical replacement or reattachment of the fragment to the adjacent bed with a pin is required when the weight-bearing surface is involved.
Prognosis
OCD lesions that occur in the first decade have a better prognosis for healing compared to lesions that occur in second decade.
Patellar Instability and Dislocation
Patellar instability and patellar dislocation may occur from a direct blow, tight lateral structures (ilitobial band or vastus lateralis), or ligamentous laxity (Ehlers-Danlos). It presents with knee instability with anterior knee pain.
Mechanism of Injury
This is typically a noncontact twisting injury with the knee extended and foot externally rotated. Patient will usually reflexively contract quadriceps subsequently reducing the patella. Osteochondral fractures frequently occur as the patella relocates.
Direct blow is a less common mechanism. Examples include knee to knee collision in basketball, or football helmet to the side of the knee.
Physical Examination
- Acute dislocation is usually associated with a large hemarthrosis. Absence of swelling supports ligamentous laxity and habitual dislocation mechanism
- Medial-sided tenderness (over medial patellofemoral ligament)
- Patellar apprehension: passive lateral translation results in guarding and a sense of apprehension
- J-sign: Examiner observes patellar deviation laterally in the shape of the letter "J" with knee extension which "pops" into groove as the patella engages the trochlea early in flexion. It is associated with patella alta (high-riding patella).

Evaluation: Imaging
- X-rays: are indicated to rule out associated fractures, which most commonly involve the medial patellar facet or lateral femoral condyle.
Views:
- AP view is best to evaluate lower extremity alignment
- Lateral view is best to evaluate trochlear dysplasia and patellar height (patella alta = high-riding patella, patella baja = low-riding patella)
- Sunrise view or Merchant view assesses lateral patellar tilt
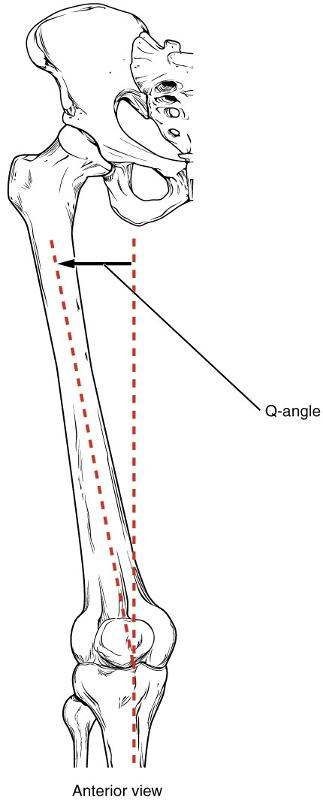
Increased Q angle: increased angle between the force vector of the quadriceps and the patellar tendon.
- MRI: is better for evaluation of suspected loose bodies, fracture on medial patellar facet, and tears of medial patellofemoral ligament
Management
- Non-operative: conservative approach include NSAIDs, activity modification, sometimes short-term immobilization with patellar stabilizing sleeve for comfort, and physical therapy for strengthening exercises and balance.
- Operative: arthroscopic debridement of loose bodies, fracture repair, or repair of ligamentous tear
QuickCheck
![]()
Image source from Widimedia Commons: https://commons.wikimedia.org/wiki/File:818_Femur_Q_Angle.jpg

