Non-Accidental Musculoskeletal Injuries
In a clinical setting where musculoskeletal injury is the chief complaint, it is imperative to maintain a threshold of suspicion for physical abuse as the primary cause of an injury. Non-accidental injuries may be difficult to recognize since caretakers rarely disclose maltreatment, some children cannot provide a history, and signs and symptoms of physical abuse may be subtle or confused with other common pediatric diagnoses.
Signs & Symptoms
- History inconsistent with injury
- Cutaneous lesion is the most common finding, including burns and bruises. Multiple bruises should raise high suspicion for non-accidental trauma.
- Fractures with high specificity for non-accidental trauma
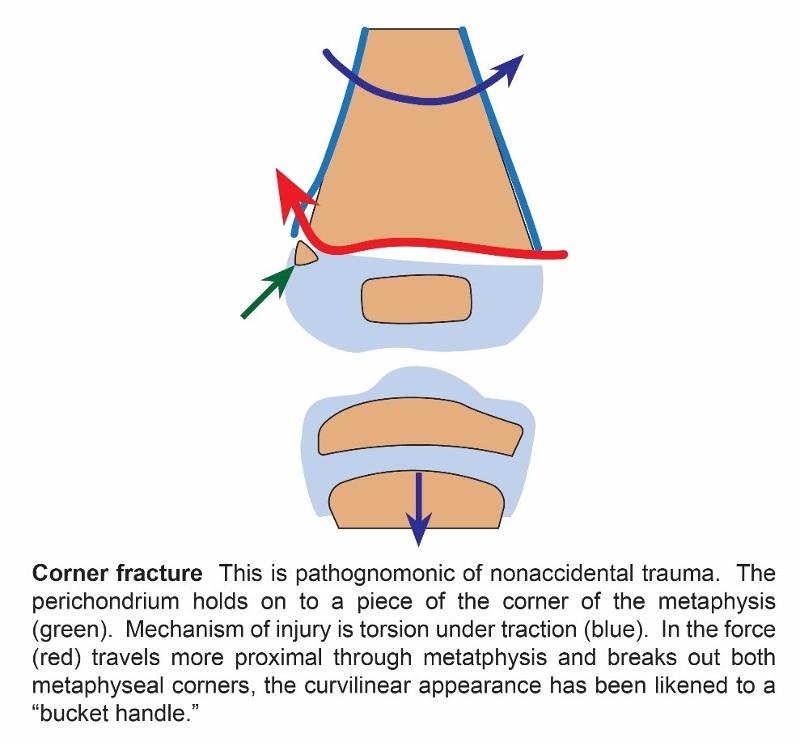
a. Corner fracture, also known as bucket handle fracture, is a metaphyseal fracture that is pathognomonic of non-accidental trauma. (see below)
|
|
|

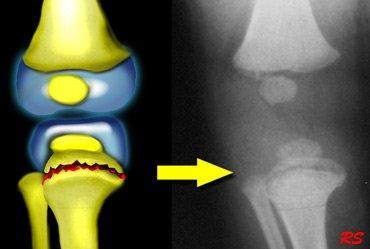
Image source: Radiology Assistant
b. Scapula fractures
c. Spinous process
d. Sternum fractures
e. Skull fractures
f. Multiple fractures in various stages of healing
g. Bilateral fractures
h. Long bone fractures (particularly femur and humerus spiral fractures) in non-mobile infants
i. Metaphyseal fractures
j. Frequency of fractures: humerus > tibia > femur
k. Diaphyseal fractures are four times more common than metaphyseal
l. Posterioir Rib Fractures (see below)

Image source: Radiology Assistant
4. Seeking medical care at different facilities for repeat events.
5. Associated risk factors for abuse include prematurity, parental youth, and unmarried status
There are medical conditions which can predispose children to have bony abnormalities making them more prone to fractures. These conditions warrant further work-up. It is important to consider these as etiology of the fracture and not exclusively from abuse.
- Osteogenesis imperfecta (particularly type IV which does not have the distinctive blue sclera)
- Osteomyelitis
- Infantile cortical hyperostosis
- Leukemia
- Hypervitaminosis A
- Rickets
Evaluation: Imaging
- X-rays: chest, skull, AP views of arms, forearms, hands, pelvis, thighs, and legs, lateral view of spine occasionally (depending on circumstance)
- Skeletal survey: should be included as part of the initial evaluation
- Bone scan: alternative or adjunct to the radiographic skeletal survey in selected cases, particularly for children older than one year of age. It provides increased sensitivity for detecting rib fractures, subtle shaft fractures, and areas of early periosteal elevation. Bone scan is not useful in metaphyseal or cranial fractures and not indicated after five years of age.
Management
Physicians are legally obligated to report suspected child abuse and neglect. Physicians are granted immunity from civil and criminal liability if they report in good faith but may be charged with a crime for failure to report.
It is important to know the law and resources specific to your state.
The Texas Abuse Hotline, via Texas Department of Family & Protective Services.
1-800-252-5400
QuickCheck


