Fractures
Overview
Physical Examination
- Visual inspection: Gross position of the extremity allows you to appreciate for presence or absence of deformity, distortion or abnormal angulation, and longitudinal shortening. Evaluate the overlying skin and soft tissues for swelling, ecchymosis, abrasions, punctures, and lacerations. Comparison with the opposite extremity and measurement of circumference can be very helpful when findings are subtle.
- Palpation and assessment of active and passive motion: localized swelling and tenderness on palpation are significant findings and should alert the examiner to the likelihood of an underlying fracture. Observe the spontaneous movement, attempts to get the patient to voluntarily move the involved part through its expected range, and passive movement. Pain on motion and limitation of motion signal the need for further examination.
- Checking neurovascular function distal to the injury is essential in evaluating any child with a potential fracture. Check the integrity of pulses and speed of capillary refill, as well as testing sensory and motor function. Assessment of two-point discrimination is probably the best test of sensory function. Evidence of neurovascular compromise necessitates urgent, often operative, orthopedic treatment.
Evaluation: Imaging
- X-Rays: At minimum, two views are obtained, taken at 90-degree angles. Radiographs should include the joints immediately proximal and distal to a fractured long bone. It isvaluable to obtain comparison views of the contralateral side, especially if there is suspected physeal injuries which may have very subtle radiographic abnormalities.
Anteroposterior (AP) and lateral views are the most common.
Oblique views are helpful for fully disclosing the nature and extent of many fracture patterns, especially when the injury involves the ankle, elbow, hand (especially for scaphoid fracture), or foot. Oblique views are also helpful for detecting subtle spiral fractures where the AP and lateral views are normal, yet a fracture is strongly suspected.
Ankle AP mortise view is helpful since it includes distal tibia, distal fibula, talus, and proximal metatarsals.
- Computed Tomography scan can be useful for displaced or angulated fractures, complex intra-articular fractures, vertebral, and pelvic fractures.
- Magnetic Resonance Imaging is most useful to evaluate associated soft tissue injury, such as spine fracture (to evaluate neural elements) or at the knee (to rule out meniscal tear in the setting of intercondylar eminence of tibia fracture). MRIs for children require sedation.
- Ultrasonography is most useful for diaphyseal fractures, particularly if further imaging decision is in question. The imprecision of ultrasonography around physes and joints limits its utility and influence on management.
- Bone scan may be useful for detecting subtle stress fractures.
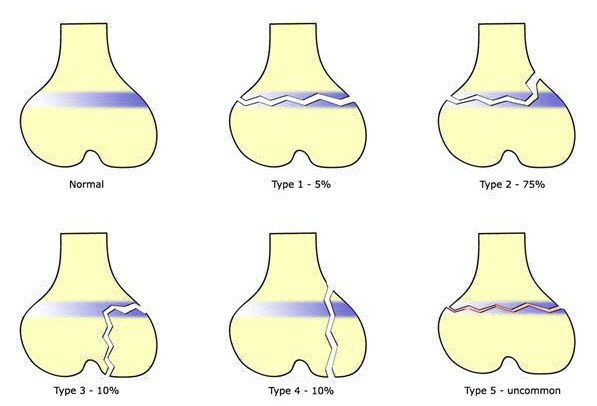
Salter-Harris Classification System
This is the standard classification system for description of fractures involving the growth plate (also called physis or epiphyseal plate).
- Types I & II have extra-articular involvement and are at-risk for growth disturbances.
- Types III & IV have articular involvement and are at-risk for growth disturbances and osteoarthritis.
Prevalence of Fracture Types Using the Salter-Harris Classification System
|
Type I Fracture through physis; extra-articular |
||
|---|---|---|
|
Salter-Harris Type I on right distal tibia |
Salter-Harris Type I on right proximal tibia |
Salter-Harris Type I on left distal radial |
|
Type II Fracture through physis and metaphysis |
||
|
|
Salter-Harris Type II on distal femur |
|
|
Type III Fracture through epiphysis and physis |
||
|
Salter-Harris Type III on distal tibia |
Salter-Harris Type III on right distal tibia |
|
|
Type IV Fracture through epiphysis, physis, and metaphysis |
||
|
|
Salter-Harris Type IV of base of proximal phalanx |
|
|
Type V Compression injury to physis without fracture. Rare and identifiable only in retrospect, when compression of the physis has led to growth disturbance. |
||
|
Salter-Harris Type V on distal tibia |
Salter-Harris V through medial aspect of left distal tibia
|
|








Fracture Patterns
1. Humerus fracture
1a. Proximal humerus fracture
Mechanism of Injury
The Mechanism of Injury is blunt trauma or indirect trauma (including overuse injury in throwers such as Little Leaguers shoulder.
Radiographs show mild widening of the physis and metaphyseal changes


Proximal humerus fracture
1b. Humerus shaft fracture
Mechanism of Injury
Often associated with trauma. Consider non-accidental trauma if less than three years of age and spiral fracture pattern.

Humerus shaft fracture
2. Elbow fractures
2a. Supracondylar fracture
Supracondylar fractures represent half of pediatric elbow fractures and most operated pediatric fracture.
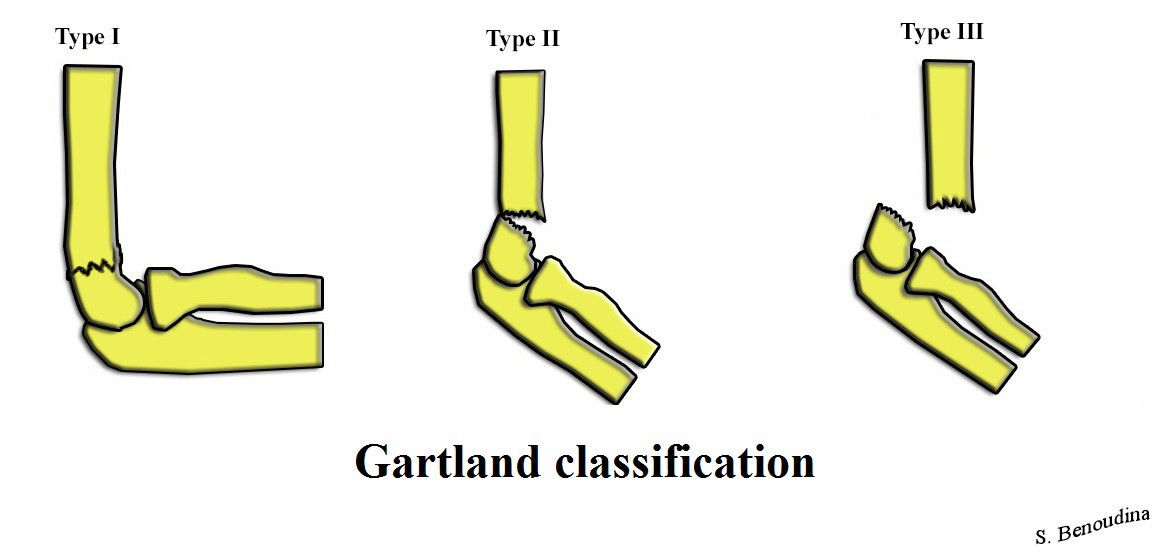
Gartland Classification of Supracondylar Humerus Fracture
Image Source from Wikimedia Commons: https://upload.wikimedia.org/Wikimedia/commons/f/fc/Gartland_Classification.jpg
Mechanism of Injury
- Extension type: (>95% of cases): Injury is often a fall onto the outstretched upper limb with the hand as the point of contact. On exam, the antecubital skin may be bruised.
- Flexion type: Mechanism of injury is a fall onto the flexed elbow with the olecranon as the point of contact.
Associated Injuries
- Neuropraxia: Nearly all cases of neuropraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies are not indicated in the acute setting. Anterior interosseous nerve neuropraxia (branch of median nerve) is the most common nerve palsy seen with supracondylar humerus fractures. On exam, the patient is unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger (cannot make A-OK sign).
Radial nerve palsy is the second most common neuropraxia. On exam, patient is unable to extend wrist or digits.
Ulnar nerve palsy is seen with flexion-type injury patterns.
- Vascular injury occurs in 1% of supracondylar fractures. Exam findings include cold, pale, and pulseless hand. Vascular compromise is a medical emergency which requires treatment with immediate reduction and pinning in the operating room.
Evaluation: Imaging
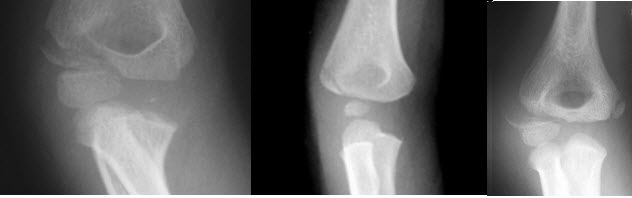
AP and lateral view of the elbow x-rays show posterior fat pad sign : lucency along the posterior distal humerus and olecranon fossa is highly suggestive of occult fracture around the elbow.

Supracondylar humerus fracture

Supracondylar humerus fracture


Supracondylar humerus fracture
Management
- Type I (non-displaced) fracture: long arm posterior splint
- Type II, III, IV: reduction and wire fixation within 24 hours of injury
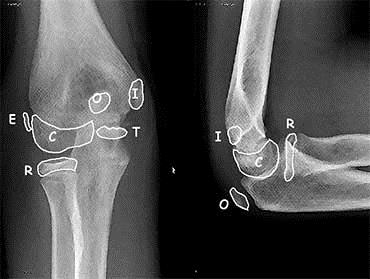
2b. Medial epicondyle fracture
Mechanism of Injury
Injury can be a fall on an outstretched arm (most common), elbow dislocation, traumatic avulsion (usually occurs in overhead throwing).
Medial epicondyle fracture
Physical Examination
Tenderness over medial epicondyle.
2c. Lateral condyle fracture
Medial epicondyle fracture
Mechanism of Injury
Results from the pull of the common extensor musculature or fall on an outstretched hand.
Physical Examination
Swelling and tenderness to the lateral elbow is notable on exam. There is also increased pain upon wrist extension or flexion.
2d. Radial head / neck fractures (of the elbow)
Mechanism of Injury
Typically involves valgus loading injury of the elbow.
Physical Examination
There is swelling over lateral elbow. Pain is exacerbated upon forearm supination and pronation. Sometimes, there is referred pain to the wrist.
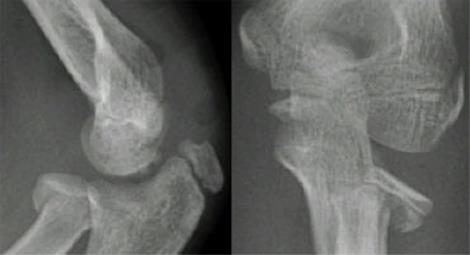
Radial head/neck fractures
3. Radius fractures
3a. Distal metaphysis (complete fracture)
Apex volar (Colles' fracture)
Apex dorsal (Smith's fracture)
3b. Distal metaphysis (incomplete fracture)
Torus/Buckle fracture (typically unicortical)
3c. Diaphysis
Plastic deformation: incomplete fracture with deforming force resulting in shape change of bone without clear fracture line, occurs along compression side.
Greenstick fracture: incomplete fracture resulting from failure along tension (convex) side.
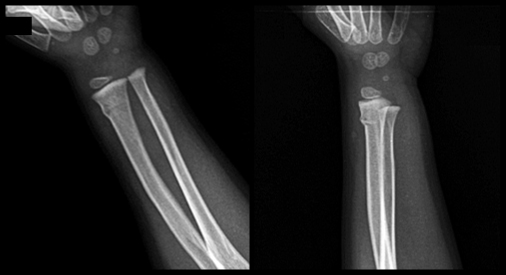
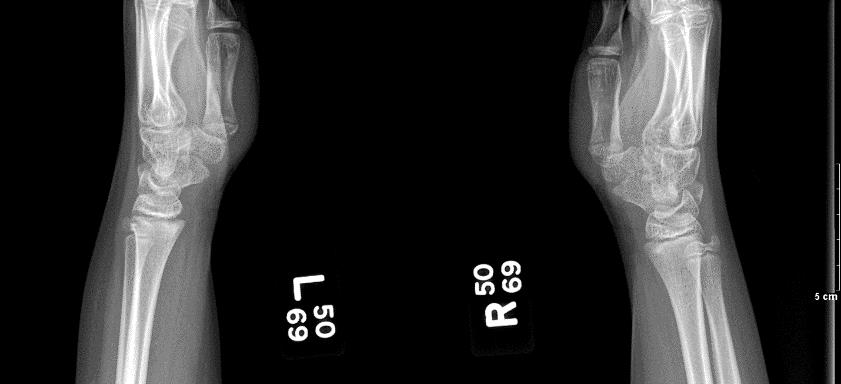
Buckle /Torus fracture of the dorsolateral cortex of the distal radial metaphysis

Plastic deformation (bowing deformity) of the right radius
and an oblique mid-diaphyseal ulnar fracture
with posterior displacement of the distal fragment (one shaft-width)
4. Femoral shaft fracture
Abuse must be considered if child is less than five years of age, especially if present in a patient before walking age. Femur fractures are the second most common child abuse associated fracture after humerus fractures. (See also the section below on Non-accidental fractures.)
Symptoms
Patients typically present with thigh pain, inability to walk, report of leg deformity or instability.
Mechanism of Injury
The mechanisms of injury is correlated with age due to the increasing thickness of the cortical shaft during skeletal growth and maturity. Falls are the most common cause in toddlers. Whereas, high energy trauma is responsible for injury in adolescents, typically from motor vehicle collision. Fractures after minor trauma can be the result of a pathologic process (bone tumors, osteogenesis imperfecta, osteopenia).
Physical Examination
Examination reveals gross deformity, swelling of the thigh, and exquisite tenderness to affected area.
Evaluation: Imaging
X-rays:
- AP and lateral views of femur typically allow complete evaluation of the fracture location, configuration and amount of displacement.
- Ipsilateral AP and lateral views of knee and hip are required to rule out associated injuries.
Management
- Non-operative intervention include long leg cast for nondisplaced femoral shaft fracture with multiple medical comorbidities.
- Operative interventions are indicated when there is a diaphyseal femur fracture or femoral neck fracture.
Complications
- Leg-Length Discrepancy: either overgrowth or shortening.
- Osteonecrosis of femoral head if femoral nailing is done through the piriformis fossa.
- Nonunion or malunion.
5. Tibia shaft fracture (Toddler fracture)
This type of fracture is also referred to as childhood accidental spiral tibial (CAST) fractures
Mechanism of Injury
The injury is low energy trauma with rotational component or hyperextension of the knee when landing from a jump.
Physical Examination
Child may limp or refuse to walk. Exam shows tenderness but no obvious swelling or deformity.
Evaluation: Imaging
X-ray may reveal nondisplaced spiral or oblique fracture (distal metaphyseal oblique proximal lateral to distal medial) of tibial shaft only. Fibula typically remains intact. Toddler fracture involves the distal half of tibia, unlike non-accidental injury, which typically involves proximal half of tibia.
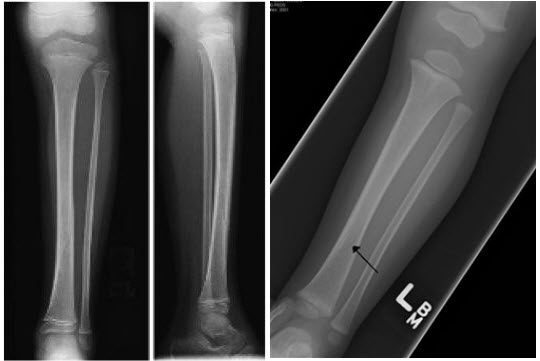
Tibia shaft fracture (Toddler fracture)
6. Stress fracture
Stress fractures most commonly affect the long bones of the lower legs (more commonly the tibia) but can also involve the foot, hip, knee, or ankle.
Mechanism of Injury
Overuse injuries commonly cause abnormal stresses on trabecular bone resulting in microfractures, which subsequently propagates within the bone. Repetitive loads then exceed the threshold of intrinsic bone healing. This is commonly seen in young athletes.
Evaluation: Imaging
X-ray may be normal. Sometimes, injuries require bone scan to confirm diagnosis.

Stress Fracture
7. Scaphoid fracture
Mechanism of Injury
Most commonly via axial load across hyper-extended and radially deviated wrist.
Physical Examination:
- Anatomic snuffbox tenderness dorsally.
- Scaphoid tubercle tenderness volarly: tenderness at the volar distal pole is more reliable than in the anatomic snuffbox.
- Pain with resisted pronation. Note guarding with wrist motion.
Evaluation: Imaging
- X-rays: AP and lateral views are the most recommended views. If further views are needed, scaphoid view (30 degree wrist extension, 20 degree ulnar deviation, 45 degree pronation view) may be beneficial. If radiographs are negative and there is a high clinical suspicion, consider repeating radiographs in 2-3 weeks.
- MRI: effective for diagnosing occult fractures less than 24 hours post-injury.
- Bone scan: effective for diagnosing occult fractures at 72 hours post-injury.
Management
- Distal pole fractures and nondisplaced waist fracture can be managed with thumb spica cast.
- Displaced wrist fracture are at risk for osteonecrosis and are treated with open reduction and internal fixation.

Scaphoid Fracture
8. Phalanx / Finger fractures
Mechanism of Injury
Trauma, including sports, is the most common cause of injury.
Physical Examination
Examination reveals localized tenderness and/or deformity. Look carefully for open wounds.
Evaluation: Imaging
Finger X-ray: Obtain AP and lateral views if there is a specific, localized area of pain.
Hand X-ray: Obtain hand x-ray if there are suspicion for carpal or metacarpal bone involvement.

Spiral Fracture on proximal phalanx of 2nd digit
Management
- Nonoperative: buddy taping with three weeks of immobilization.
- Operative indications.
- Irreducible, unstable, or transvers fracture patterns.
- Distal phalanx fracture associated with a nailbed injury.
Splinting
Goals of splinting
- Decrease pain
- Mechanical stabilization of bones, soft tissues, and neurovascular structures
- Decrease risk of further injury to the affected area
- Decrease risk of additional swelling-related injuries such as compartment syndrome
- Splint is advantageous for immobilization, especially if more swelling is anticipated prior to placement into a cast.
Equipment
- Fiberglass (Ortho-Glass) is becoming the standard because it is less messy and lighter.
- Ace wrap
- Crutches or arm sling
- Water basin
- Dry towel
|
TYPES OF SPLINTS |
|
|---|---|
|
Splints for |
Indication |
|
Bulky hand compression dressing |
Closed hand fractures |
|
Colles splint |
Distal forearm and wrist fractures |
|
Dorsal or volar splint |
Wrist fractures or injuries, fractures of 2nd - 5th metacarpals, soft tissue injuries of the hand |
|
Figure-of-eight splint |
Medial clavical fractures |
|
Gutter splint |
Phalangeal and metacarpal fractures |
|
Posterior arm splint |
Stable elbow and forearm injuries |
|
Sling and swathe |
Shoulder injuries, humeral injuries |
|
Sugar tong splints |
|
|
Proximal |
Humeral fractures |
|
Distal |
Wrist fractures, distal forearm fractures |
|
Double |
Elbow fractures, forearm fractures |
|
Reverse |
Distal forearm fractures |
|
Thumb spica splint |
Scaphoid fractures, extra-articular fractures of the thumb metacarpal, ulnar collateral ligament injuries |
|
Velpeau bandage |
Shoulder injuries, humeral injuries |
|
Volar finger splint |
Fractures of distal phalanges and interphalangeal joints |
|
Splints for |
Indication |
|
Buddy taping |
Phalangeal fractures of the toes |
|
Bulky foot compression dressing |
Calcaneal fractures; foot injuries |
|
Jones compression E |
Knee and calf injuries |
|
Knee splint |
Knee injuries |
|
Posterior ankle splint |
Distal leg, ankle, tarsal, and metatarsal fractures; reduced dislocations; severe sprains |
|
Stirrup splint |
Ankle fractures |
![]()
Applying a Distal Sugar Tong Splint
a 7 minute video by S. Sanchez, UTMB
Compartment Syndrome
The muscle groups are divided in compartments and bound by rigid fascial membranes. Compartment syndrome occurs when increased pressure within a closed fascial compartment (often due to bleeding and edema collection) causes neurovascular compromise and muscle ischemia. Increased pressure, exacerbated by capillary leaking, first occludes venous outflow and only later occludes arterial flow to produce the classic signs and symptoms. Compartment syndrome is defined as pressure greater or equal to 30 mm Hg.
Symptoms: paresthesia and intense pain (aggravated by passive stretching of the muscles).
Signs: affected area is swollen & tense, pallor, and decreased pulses.
Common fractures prone to compartment syndrome
- Supracondylar fracture
- Forearm fractures (more commonly with distal radius)
- Tibial fracture (usually diaphysis)
- Minor fractures of the tibia, radius, ulna, metatarsals, and femur
Other Complications Due to Fractures
Penetrating injuries
Fractures may cause penetrating injuries to surrounding structures. Any overlying bony structures, if bloody and fatty exudate is oozing, usually reflect communication with the medullary cavity of a fractured bone.
In the knee joints, if serous or serosanguineous fluid flows during knee movement, this is suggestive of a penetration of the joint capsule. Air seen in the radiograph of the knee joint confirms the diagnosis. Absence does not rule out capsular penetration, but warrants exploration in the OR.
Neurovascular injury
Neuropraxia is a type of peripheral nerve injury that is classified as a transient conduction block of motor or sensory function. Although nerve degeneration does not occur, there can be a loss of motor function. Patients are usually able to fully recover within a period of weeks to months.
Although vascular injury can occur, there is rich collateral circulation that can maintain circulation.
Fractures associated with neurovascular injury include:
- Supracondylar fractures of the humerus
- Fractures of the distal femoral shaft
- Severely displaced ankle fractures
Additional Complications
- Slowing or arrest of growth of bone if injury involves the growth plate
- Reduction in bone mineralization making it more susceptible to injury
- Salter Harris Type III & IV fractures have articular involvement and are at-risk for osteoarthritis.
- Tendon laceration in hand injuries. Complete laceration exhibits no resting flexor tone.
QuickCheck

