
All pregnant mothers hope for the healthy, full-term delivery of their baby. But for many mothers, that's not how things go.
There are over 15 million pregnancies a year in the U.S., and each year,
over a million of those babies do not survive complications caused by
premature birth. And to make matters worse, the rate of pre-term birth, which is defined as birth before 37 weeks’ gestation, has not changed in over 35 years.
“It’s a major problem around the world, but the U.S. has a very high rate of premature birth,” said Dr. Ramkumar Menon, director of UTMB Obstetrics and Gynecology’s Division of Basic Science and Translational Research. “About 10.5% of pregnancies are impacted by pre-term birth here, and there’s a huge racial disparity—17% of African Americans have pre-term births, regardless of socio-economic status. We have not addressed this problem.”
Menon said he became passionate about the field of perinatology, the branch of obstetrics that focuses on the period of time around childbirth, as a graduate student at Wright State University in Dayton, Ohio.
He was looking for a research project to work on and ended up being mentored by a renowned perinatologist, who chose him to work on a study focused on the causes of premature birth and guided him to use fetal membrane tissue as a model for his work.
“That was the time that I discovered a lot of things, and perinatology became my passion,” he said. “I learned about the importance of collaborative research, and the need to advance translational research—it must benefit someone at the end of the day.
“If it doesn’t help a person in need, then what is the reason for it? I learned the impact of translational research, and I have been following it ever since.”
Yet, over three decades since studying at Wright State, Menon said there are few new therapies or medicines to help prevent pre-term labor.
“The problem is, we do not have a good model to study,” he said. “You develop a drug, you test it in every lab model you can use, and every animal model. You take all your great data to the FDA, and they will still say you have not recreated a human pregnancy.”
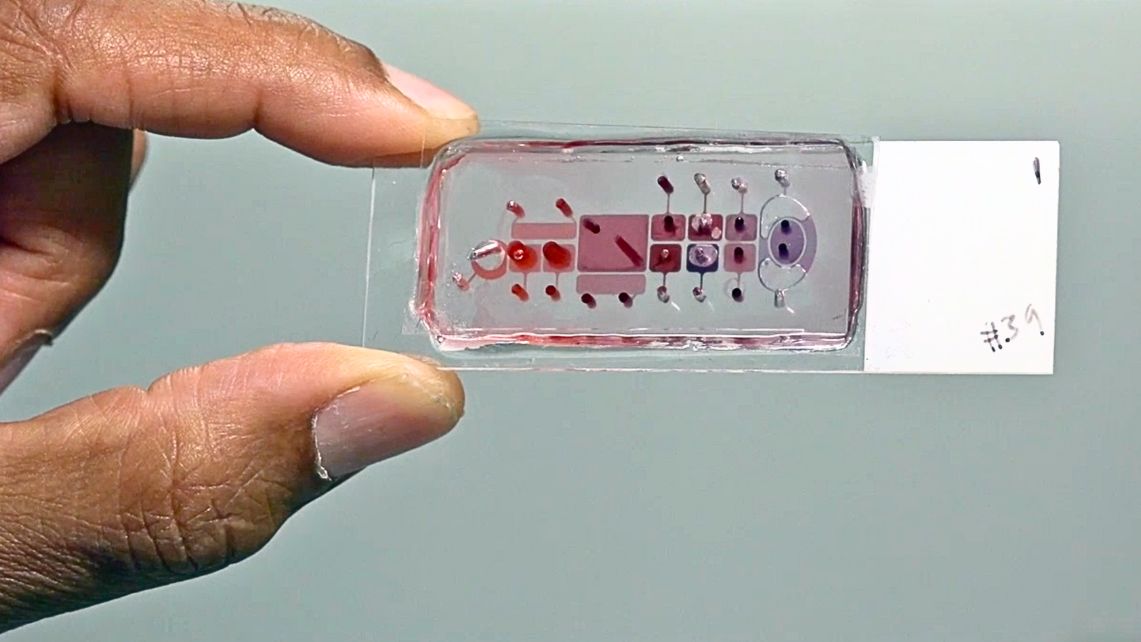 This is why the goal of the Menon Laboratory for Perinatal Research is to create humanized pregnancy models that simulate a mother and fetal system as a single unit in the lab. He explained that with a pregnant woman, there are two patients in one body, and doctors are currently restricted to treating the mother. Menon and his lab are able to study gestational disease thanks to a breakthrough that mimics pregnancy using
miniature organ models made up of human cells embedded onto silicon
surfaces.
This is why the goal of the Menon Laboratory for Perinatal Research is to create humanized pregnancy models that simulate a mother and fetal system as a single unit in the lab. He explained that with a pregnant woman, there are two patients in one body, and doctors are currently restricted to treating the mother. Menon and his lab are able to study gestational disease thanks to a breakthrough that mimics pregnancy using
miniature organ models made up of human cells embedded onto silicon
surfaces.
“The fetus and the mother are communicating all the time, and it’s required for the development of the baby,” Menon said. “We discovered in my lab that there are small nanoparticles called extra cellular vesicles, or exosomes, that go back and forth between mother and fetus. Each produces them and sends them to the other.”
These particles, he continued, are cargo-carrying messages. They can be proteins, nucleic acids, lipids, or anything.
“That’s the message going back and forth,” he said. “It is decoded by the recipient’s cells, and that translates into action. If the mother is getting vesicles loaded with inflammation, the fetus will respond by saying it has complications or an infection. Mother can respond.”
By looking at both the mother and the fetus as patients, it’s possible to enclose a drug in the extra cellular vesicle and treat the mother and the patient at the same time. The fetus can develop inflammation through some exposure of the mother to an infection or other risk factors during pregnancy, and the fetus is responding, which is what needs to be controlled.
“The fetus is also a patient, and it can trigger the process of delivery. It’s possible to stop the fetus from sending the wrong signals at the wrong time and stay in for at least 37 weeks,” he said. “There is a question of whether it’s safe for a fetus to stay in an environment that is not good. We can force the baby to be delivered if that’s the case, but if we have a drug to treat the baby, or reverse the unsafe environment through treatment, we can treat the inflammation, which is the condition that normally triggers the cascade of events that results in delivery.”
 Over 60% of preterm babies are due to these infectious and inflammatory triggers. Menon’s lab has designed an anti-inflammatory drug packed inside the extra cellular vesicles. The drug, which contains a protein that already exists in the body naturally and can be grown in the lab, supplements the protein levels that drop too low in the fetus, making it impossible to fight the infection. The drug is in the developmental process, having been tested successfully on multiple platforms. The last phase of testing is on a primate model, a project recently funded by the National Institutes for Health.
Over 60% of preterm babies are due to these infectious and inflammatory triggers. Menon’s lab has designed an anti-inflammatory drug packed inside the extra cellular vesicles. The drug, which contains a protein that already exists in the body naturally and can be grown in the lab, supplements the protein levels that drop too low in the fetus, making it impossible to fight the infection. The drug is in the developmental process, having been tested successfully on multiple platforms. The last phase of testing is on a primate model, a project recently funded by the National Institutes for Health.
“It’s my hope that this work is life changing,” he said. “It’s all about saving babies. This is our tagline—it’s about saving babies.”