

Tricuspid Atresia (TA)
TA is a rare form of CHD (1% of all CHD). The RV is hypoplastic and an ASD is necessary for survival. If the ventricular septum is intact, the pulmonary valve would also be atretic. If a VSD is present, there will be a variable degree of hypoplasia of the pulmonary valve depending on the size of the VSD.
TA is classified according to the presence or absence of VSD or TGA. In one fourth of the patients, there is a TGA. Patients with TA with normally related great vessels may be more cyanotic than those with TGA as the degree of cyanosis is inversely related to the volume of the pulmonary blood flow (Figures).
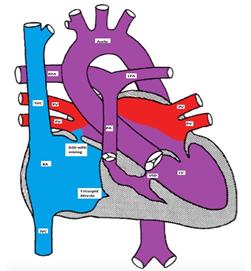
Figure showing tricuspid atresia with a restrictive VSD, pulmonary hypoplasia and normally related great arteries
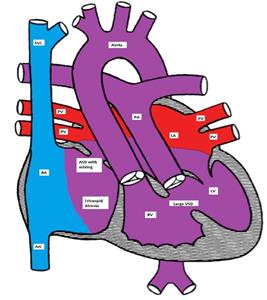
Figure showing tricuspid atresia with a non-restrictive VSD and d-TGA
Clinical presentation, EKG and, imaging
Patients with TA are cyanotic and have a single S2. A holosystolic murmur of VSD may be heard. A PDA murmur may also be heard.
EKG classically shows a left superior axis deviation (due to posterior and inferior displacement of AV node) and diminished RV forces. LVH may be present. Echo is usually diagnostic.

EKG showing superior left axis deviation and reduced right ventricular forces consistent with tricuspid atresia
Management
Management includes IV infusion of PGE-1 to maintain the ductal patency. CHF needs to be treated if present. Rashkind atrial septostomy may be needed if the ASD is restrictive. Patients with TGA and hypoplastic RV will need multi-stage single ventricle repair (see Fontan-type operation in HLHS).
Pulmonary Atresia with Intact Ventricular Septum (PA-IVS)
PA with IVS occurs in 2.5 % of patients with CHD.
There is no direct communication between the RV and the main pulmonary artery (MPA) as the pulmonary valve is atretic. The RV is usually hypoplastic. An atrial communication is needed for survival. The pulmonary blood flow is dependent on the patency of the ductus arteriosus.
Clinical presentation, EKG, imaging
Clinically, patients are severely cyanotic and have respiratory distress. The S2 is single and a PDA murmur may be heard. EKG shows RAE, LVH and possibly RVH.
CXR usually shows reduced pulmonary vasculature.
Management
- PGE-1 should be started to maintain the ductal patency.
- Cardiac catheterization is usually needed for the evaluation of the type of PA (membranous vs. muscular) and to detect the presence of coronary sinusoids.
- Balloon atrial septostomy may be performed in the cardiac cath lab.
- Perforation of a membranous atretic pulmonary valve (by radiofrequency) may be attempted.
- If the RV size is adequate, trans-annular patching across the pulmonary outflow may be done.
- In patients with RV dependent coronary circulation, RV decompression may lead to reversal of the coronary blood flow to the RV producing myocardial ischemia. In this case, a BT shunt is placed in preparation for a single ventricle repair.
Ebstein Anomaly of the Tricuspid Valve (EA)
Ebstein anomaly is a rare form of CHD (1%).
There is a downward displacement of the septal and posterior leaflets of the tricuspid valve into the RV cavity creating a large atrialized portion of the RV. The functional RV may be hypoplastic, dilated and thin-walled. There is usually an inter-atrial communication such as PFO or ASD. Ebstein anomaly may be associated with other CHD such as PS, TOF, pulmonary atresia, VSD.
Dysrhythmias, especially Wolff-Parkinson-White (WPW) and SVT are commo
Figure showing Ebstein Anomaly of the tricuspid valve
Clinical presentations, EKG, imaging
Infants may present with cyanosis which usually improves as the pulmonary vascular resistance drops. Older children usually present with dyspnea, fatigue and palpitations (SVT). A quadruple rhythm may be audible in addition to a holosystolic murmur at the left lower sternal border due to tricuspid insufficiency. A mid-diastolic murmur due to relative tricuspid stenosis may be heard at the same location. EKG is characterized by massive right atrial enlargement (RAE), RBBB and sometimes first degree AV block or WPW. CXR shows cardiomegaly due to RAE. Echocardiogram is diagnostic. The degree of TR and the size of the RV should be determined.
Management
Medical management is recommended in mild forms. This includes management of CHF and treatment of dysrhythmias. Oxygen supplementation is helpful early in life as it decreases the pulmonary vascular resistance. PGE-1 may be needed to maintain the ductal patency in severe cases. Surgery is required for severe forms and involves reconstruction or replacement of the tricuspid valve and closure of the ASD. If the RV is severely hypoplastic, a single ventricle repair (Fontan procedure) may be necessary.
Hypoplastic Left Heart Syndrome
Hypoplastic Left Heart Syndrome (HHLS) occurs in about 1% of CHD and involves hypoplasia or atresia of the left sided structures including the LA, mitral valve, LV, aortic valve and ascending aorta (Figure). A shunt at the atrial level (ASD or PFO) is necessary for survival. A PDA is essential for providing blood supply in a retrograde direction to the transverse and ascending aorta to provide blood to the neck vessels and coronary arteries.
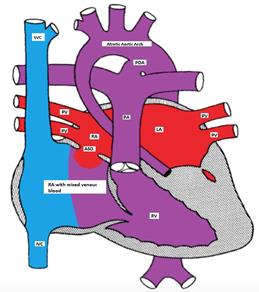
Figure showing hypoplastic left heart with a non-restrictive ASD and a PDA
Pathophysiology
There is an obligatory L to R shunt at the atrial level. Both pulmonary and systemic venous blood completely mix in the RA. The RV pumps blood to both systemic and pulmonary circulations. Initially, both resistances are nearly equal and the blood is distributed equally to the pulmonary and systemic circulations. As the pulmonary vascular resistance drops in the first few days of life, more blood flows to the lungs causing pulmonary congestion, reduced systemic flow causing tissue hypoxemia, metabolic acidosis, shock or even death.
Clinical presentations
Neonates with HLHS usually present with one of three clinical scenarios:
- Respiratory distress due to pulmonary congestion as the pulmonary vascular resistance drops in the first few days of life
- Shock as the ductus arteriosus constricts
- Cyanosis which is usually mild due to excessive pulmonary flow. Severe cyanosis is uncommon and may indicate inadequate inter-atrial communication or persistent pulmonary hypertension.
A systolic ejection murmur may be heard at the ULSB due to increased flow through the pulmonary valve. A holosystolic murmur due to tricuspid insufficiency may be heard at the LLSB. S2 is usually loud and single. The peripheral pulses may be weak and the skin may be mottled due to poor tissue perfusion.
Making the Diagnosis
- This condition can be diagnosed prenatally as early as 16 weeks of gestation.
- EKG: EKG findings are nonspecific and may show poor progression of LV forces and myocardial ischemic changes.
- Echocardiography is diagnostic and also helps to determine the size of the inter-atrial communication, the patency of the ductus arteriosus, RV function and the presence of tricuspid insufficiency.
- CXR shows cardiomegaly, pulmonary venous congestion and pulmonary edema.
- Cardiac catheterization is rarely necessary for diagnosis but may urgently be needed to perform balloon atrial septostomy if the ASD is restrictive.
Management
Medical management:
- PGE-1 should be started to maintain the ductal patency.
- Avoid oxygen supplementation because it causes pulmonary vasodilatation and lowers the PVR, which makes pulmonary congestion and CHF worse. This may also compromise the systemic blood flow as oxygen is a systemic vasoconstrictor.
- Avoid administration of excessive IV fluids as most of the fluid will go to the lungs.
- Also avoid high doses of inotropic agents as this causes systemic vasoconstriction and increases the SVR. This may accentuate tissue hypo-perfusion and metabolic acidosis. It also increases the myocardial oxygen demand increasing the contractility.
Surgical management: both multi-stage palliative surgery and heart transplantation have comparable outcomes.
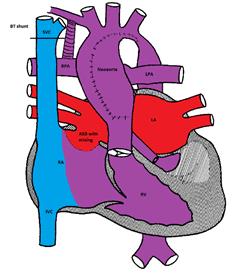
Figure demonstrating the Norwood procedure
The first stage (Norwood procedure) is performed in the neonatal period and involves division of the main pulmonary artery and ligation of the ductus arteriosus, removal of the atrial septum and reconstruction of a new ascending aorta using the proximal main pulmonary artery and the ascending aorta. A Gore-Tex® shunt (BT) is placed between the innominate artery and the right pulmonary artery to supply blood to both lungs. Because there is complete mixing of blood in the RV, the oxygen saturation is usually in the low 80's%.
Figure demonstrating the Bidirectional Glenn procedure
The second stage is called bi-directional Glenn or hemi-Fontan procedure and is usually performed at 6 months of age. The SVC is connected to the right pulmonary artery and the BT shunt is removed. The systemic venous blood from the SVC is the only source of pulmonary circulation. The IVC venous blood mixes with the pulmonary venous blood in the RV. The systemic saturation is usually in the mid to high 80's%.
Figure demonstrating the Modified Fontan procedure
The third stage is the Fontan procedure which is usually performed at 18-24 months of age. It involves connecting the IVC to the right pulmonary artery. After this procedure, both systemic and pulmonary circulations are separated. The systemic venous blood from the SVC and IVC passively flows to both lungs via the pulmonary arteries. The RV acts as the systemic ventricle. The oxygen saturation is usually in the low to mid 90% (as there is still some mixing from the coronary venous blood via the coronary sinus).
The Fontan procedure has many complications including an increase in systemic venous pressure, development of chylothorax, and diaphragmatic and vocal cord paralysis. Other complications include atrial tachy-arrhythmias, sick sinus syndrome and protein-losing enteropathy.
Surgical management of HLHS:
The first stage (Norwood procedure) is performed in the neonatal period and involves division of the main pulmonary artery and ligation of the ductus arteriosus, removal of the atrial septum and reconstruction of a new ascending aorta using the proximal main pulmonary artery and the ascending aorta. A Gore-Tex® shunt (BT) is placed between the innominate artery and the right pulmonary artery to supply blood to both lungs. Because there is complete mixing of blood in the RV, the oxygen saturation is usually in the low 80s%.(Figure)
The second stage is called bi-directional Glenn or hemi-Fontan procedure and is usually performed at 6 months of age. The SVC is connected to the right pulmonary artery and the BT shunt is removed. The systemic venous blood from the SVC is the only source of pulmonary circulation. The IVC venous blood mixes with the pulmonary venous blood in the RV. The systemic saturation is usually in the mid to high 80s%. (Figure)
The third stage is the Fontan procedure which is usually performed at 18-24 months of age. It involves connecting the IVC to the right pulmonary artery. After this procedure, both systemic and pulmonary circulations are separated. The systemic venous blood from the SVC and IVC passively flows to both lungs via the pulmonary arteries. The RV acts as the systemic ventricle. The oxygen saturation is usually in the low to mid 90% (as there is still some mixing from the coronary venous blood via the coronary sinus). (Figure)
The Fontan procedure has many complications including an increase in systemic venous pressure, development of chylothorax, and diaphragmatic and vocal cord paralysis. Other complications include atrial tachy-arrhythmias, sick sinus syndrome and protein-losing enteropathy.
![]()
