

Cyanotic Cardiac Lesions
Complete Transposition of the Great Arteries (D-TGA)
Anatomy
In D-TGA, the aorta is positioned anterior and to the right of the pulmonary artery (instead of the normal right posterior relationship). (Figure) The aorta is connected to the right ventricle and the pulmonary artery is connected to the left ventricle.
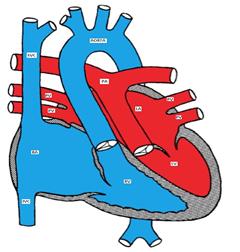
Figure showing d-transposition of the great arteries (D-TGA)
Although D-TGA is not the most common cyanotic CHD, it is the most common cardiac cause of neonatal cyanosis. It is more common in male infants of diabetic mothers who are usually large for gestational age (happy chubby blue boy).
Pathophysiology
The blood runs in two parallel circulations (rather than the normal series circulation). This situation is incompatible with life unless there is mixing between the two circulations. The mixing may occur at the atrial level (ASD or PFO), ventricular level (VSD) or at the arterial level (PDA). The atrial level communication is the most important as a bidirectional shunt can easily be produced due to the low pressure difference between the two atria as compared to the ventricles or the great arteries.
Clinical presentation
The physical examination is usually benign except for severe cyanosis and a single loud S2.
Making the Diagnosis
- EKG usually shows right axis deviation and right ventricular hypertrophy (RVH).
- CXR may show the characteristic egg on a string appearance (the great arteries lose their normal criss-cross relationship and the thymus may be hypoplastic).
- Echocardiogram is diagnostic of D-TGA. Echo is also important for identifying sites of communications between the two circulations and in delineating the coronary artery anatomy which is important in the surgical repair.
- Cardiac catheterization may be needed to perform atrial septostomy, (which could also be done under echo guidance) to allow mixing at the atrial level.
Management
Medical management includes starting PGE1 to keep the ductus arteriosus open and treatment of metabolic acidosis if present.
Surgical repair options include (Figures):
Arterial switch (Jatene) procedure in which the great arteries are switched back to the corresponding ventricle and the coronary arteries are reimplanted in the neo-aorta.
Atrial switch (Senning or Mustard) procedure involves redirecting the blood flow at the atrial level so the pulmonary venous blood is baffled to the right ventricle (systemic ventricle) and the systemic venous blood is directed to the left ventricle (pulmonary ventricle). It is a less favorable surgery because of its numerous complications.
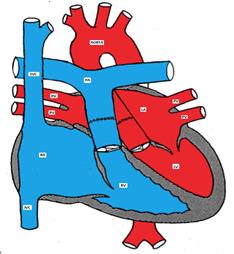
Figure showing D-TGA after arterial switch surgery.
Normal pulmonary and systemic circulations are established.
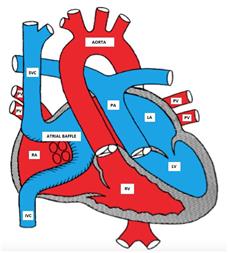
Figure showing D-TGA after atrial switch surgery
