


Pediatric Dyslipidemia
Lipids are organic and water insoluble compounds and include fatty acids, triglycerides, and cholesterol. Lipoproteins (LDL, IDL, VLDL, HDL, and chylomicrons) are soluble lipid or fat proteins that facilitate lipid movement within the aqueous environment of the body.
After digested fat is absorbed, chylomicrons are produced in the intestinal lumen and then transferred to adipose tissue, muscle, and the liver. There chylomicrons will be hydrolyzed to free fatty acids or VLDL that in turn will be metabolized to LDL (the major carrier of cholesterol to tissues). HDL acts as a "bad fat" scavenger, transferring excess cholesterol from peripheral tissues to cells that require it or to the liver to be excreted. Any abnormalities in these pathways or metabolism can lead to lipid disorders.
Etiology: The prevalence of dyslipidemia in children age 12-19 was reported as approximately 20.3% in the CDC Morbidity and Mortality Weekly Report. The most common etiology of dyslipidemia is exogenous (usually due to excessive simple carbohydrate and saturated fat intake with limited physical activity). Other etiologies include genetic (familial hypertriglyceridemia, familial hypercholesterolemia, familial defective apoB100, familial combined hyperlipidemia etc.), drug-induced (glucocorticoids, isotretinoin, protease inhibitors, immunosuppressives, beta blockers), and endocrinopathies (hypothyroidism, hyperthyroidism, T2DM, Cushing Syndrome).
Symptoms: usually associated with obesity and acanthosis nigricans. Hypertriglyceridemia may be associated with lipemia retinalis and cutaneous eruptive xanthomata. Hypercholesterolemia can be associated with xanthelasmas, corneal arcus, and tuberous xanthomata.
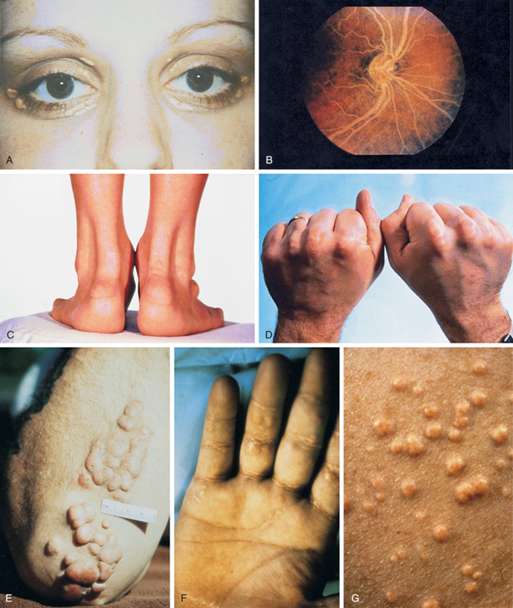
Figure 18 - Physical examination findings associated with hyperlipidemia.
From Williams Textbook of Endocrinology by Shlomo Melmed, pg. 1678.
A, Xanthelasma. B, Lipemia retinalis. C, Achilles tendon xanthomas. Notice the marked thickening of the tendons.
D, Tendon xanthomas. E, Tuberous xanthomas. F, Palmar xanthomas. G, Eruptive xanthomas.
Diagnosis: Universally screen children aged 9-11 years with a non-fasting or fasting lipid profile. A diagnosis of dyslipidemia is made with total cholesterol greater than 169 mg/dL, LDL greater than 109 mg/dL, non-HDL greater than 119 mg/dL, Apo-B greater than 89 mg/dL, triglycerides greater than 74 mg/dL in children aged 0-9 years or greater than 89 mg/dL in children older than 9 years old, or HDL less than 45 mg/dL
Treatment: diet (CHILD-1 and CHILD-2) and lifestyle changes is the mainstay. Statins are considered for cases of severe hypercholesterolemia or moderate hypercholesterolemia with risk factors/comorbidities if there is no response to a minimum of 6 months of diet and lifestyle intervention.

