



Thyroid disorders
Thyroid hormone is very important for the regulation of body metabolism and thermogenesis throughout life but it is of most critical importance for CNS development in the fetal and postnatal periods (especially the first 3 years of life). Thyroid hormone production is under the control of hypothalamic TRH and pituitary TSH but also iodine availability.
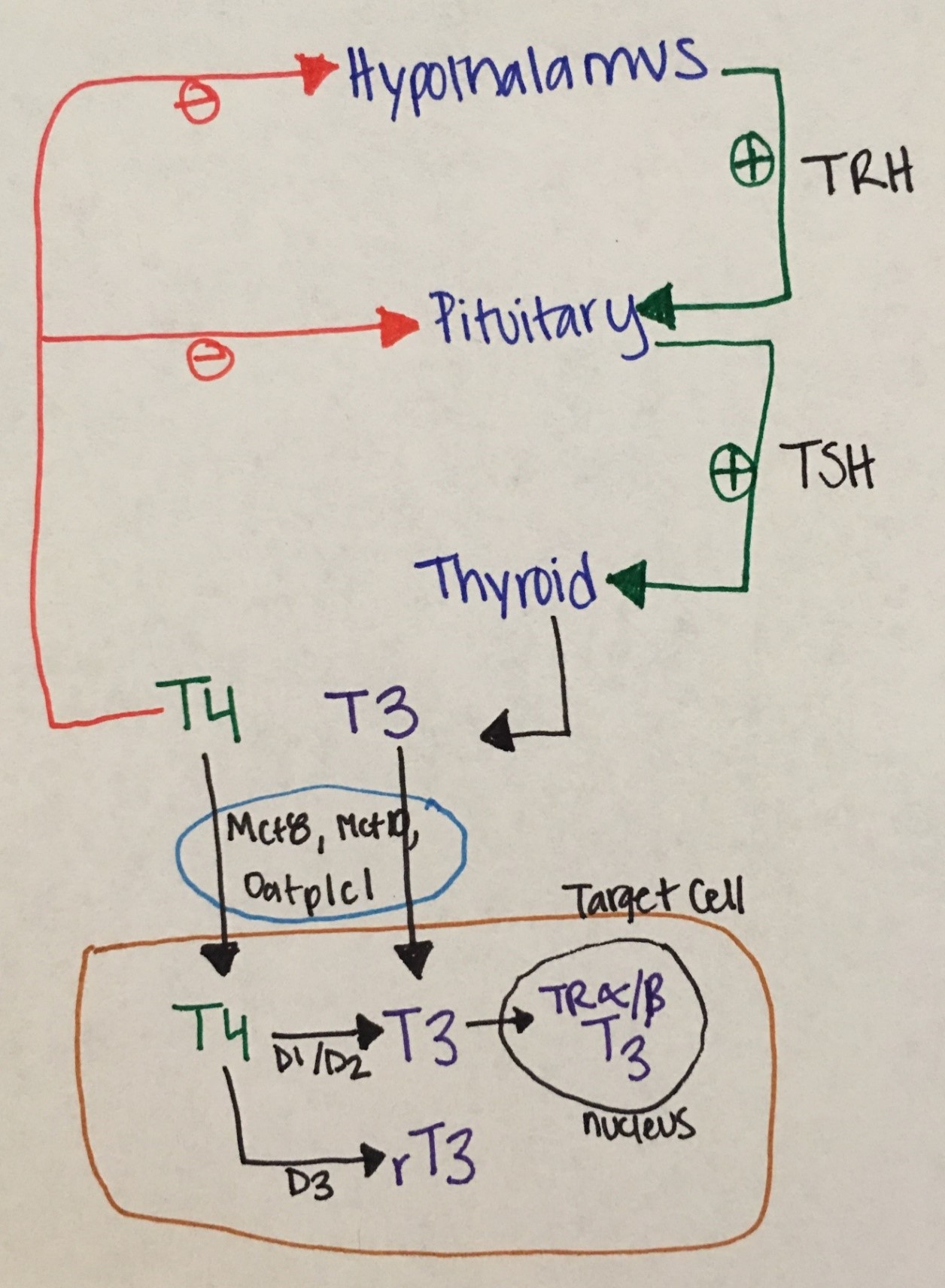
Figure 8. Phathophysiological Aspects of Thyroid Hormone Disorders/thyroid Peroxidase Autoantibodies and Reproduction
Fetal thyroid development: The fetal thyroid gland arises from an outpouching of the foregut and develops at the base of the tongue from where it will migrate down to its permanent location (over the thyroid cartilage) between the 4-8th weeks of gestation. It begins to concentrate iodine at about 10 weeks and hypothalamopituitary axis control is established at 18 weeks. Fetal T4 and TSH gradually rise to reach adult levels by 36 weeks of gestation. The rise in fetal serum T3 is less pronounced due to placental and fetal deiodeinases that covert T4 to the inactive hormone reverse T3 (rT3).
In response to the stress of birth and ambient temperature changes in the first 24 hours of life, TSH peaks up to 80 mIU/mL, driving T4 and T3 increases. Then all thyroid indices gradually normalize within the next several weeks (typically 4-6). Prematurity and perinatal complications may affect this normal process, resulting in delayed TSH rise or lower than expected T3/T4 levels.
Hypothyroidism (low thyroid hormone secretion)
Etiology: congenital vs acquired.
Congenital hypothyroidism (CH) is most commonly secondary to dysplasia/ hypoplasia of the thyroid gland or ectopia. In a minority of newborns, hypothyroidism is secondary to a defect in the synthesis of thyroid hormones (dyshormonogenesis), CNS/hypothalamic disorders affecting TRH or TSH synthesis, exposure to maternal antithyroid medication or as a result from transplacental transfer of TSH-receptor blocking antibodies. Outside the United States, the most common etiology of CH is iodine deficiency (or endemic goiter). Iodization of salt has significantly reduced CH in the United States.
Acquired hypothyroidism is most commonly due to Hashimoto thyroiditis, a destructive autoimmune disease in which there is lymphocytic infiltration of the thyroid gland. Other causes include post-surgical hypothyroidism (due to thyroid gland removal for hyperthyroidism or thyroid nodules/cancer), sick euthyroid syndrome, and subacute / suppurative thyroiditis. In autoimmune hypothyroidism (as also seen in autoimmune hyperthyroidism), children typically have a history or family history of autoimmune disease.
Symptoms:
Most newborns with CH appear normal at birth, unless mother was hypothyroid in which case babies may present with signs and symptoms of CH including jaundice (due to indirect hyperbilirubinemia), dry and coarse skin, umbilical hernia, constipation, thick protuberant tongue, poor muscle tone, anemia, hoarseness, growth retardation, delayed ossification and delayed closure of the anterior fontanel. Thyroid gland enlargement (goiter) is not usually present unless there is dyshormonogenesis. If babies with CH remain untreated, intellectual disability may ensue.
Children and teens with acquired hypothyroidism may present with decreased linear growth or even stunted growth, cold intolerance, constipation, dry skin, hair thinning or hair loss, sleepiness or irregular periods. A goiter and slow deep tendon reflexes may be present on exam. Delayed bone age maturation is also typically seen.
Diagnosis
- Newborn screen in the United States (TSH, T4 or combination of TSH and T4 depending on the state program)
- Thyroid function studies typically show an elevated TSH and low free and total T4 or T3.
- Thyroid ultrasound may demonstrate a hypoplastic or absent thyroid gland.
- Nuclear medicine thyroid scan may also be indicated in cases of suspected ectopic gland or dyshormonogenesis. In cases of autoimmune hypothyroidism thyroid peroxidase and thyroglobulin antibodies may be positive.
Treatment includes levothyroxine. Dose and monitoring schedule is variable based on age of child. For newborns, dose is ~ 10-15 mcg/kg/day. Goal of treatment is to keep free T4 levels above the mean reference range with suppressed TSH.
Hyperthyroidism (excessive thyroid hormone secretion)
Etiology. The most common etiology is Graves' disease (autoimmune stimulatory condition). Other rare causes include neonatal thyrotoxicosis due to maternal Graves' disease, activating TSH receptor mutation, and thyrotoxicosis as seen in the context of McCune-Albright Syndrome. Hot thyroid nodules are very rare in pediatrics.
Symptoms: include weight loss despite hyperphagia, palpitations, heat intolerance, increased perspiration, fatigue, diarrhea, hand tremor, anxiety and restlessness, goiter, rapid linear growth, irregular menses, and exophthalmos.
Diagnosis: TSH is typically suppressed (< 0.02 mIU/mL) and free T4, total T4 and T3 are elevated. Thyroid stimulating immunoglobulin is typically elevated.
Treatment: anti-thyroid drugs, radiation ablation (RAI) therapy or thyroidectomy. Beta- blockade is also typically necessary to decrease cardiac work.
Thyroid nodules
Thyroid nodules are uncommon (incidence 1-1.5 %). Risk factors include female sex, pubertal age, medial or family history of thyroid disease. These typically present with an asymptomatic movable, soft and non-tender thyroid mass.
Thyroid cancer
Thyroid cancer rare in children, typically presents with a painless or tender thyroid mass that is hard and fixated and associated with painless palpable neck lymphadenopathy. Distant metastases (neck, lungs, bones) are frequently present at the time of diagnosis, but survival/prognosis is excellent if early diagnosis and appropriate treatment are established. The most common type is papillary thyroid carcinoma (PTC). Follicular carcinoma is the second most common type of and is more prevalent in iodine-deficient regions. Medullary thyroid carcinomas are very rare and also the most aggressive, occurring most commonly as part of the familial MTC syndromes (e.g. MEN type 2A, MEN 2B, Carney complex etc.). The biggest risk factor is radiation exposure outside the familial cases.

