



Polyendocrinopathies
There are syndromes with a constellation of multiple endocrine diseases termed polyendocrinopathies.
Autoimmune Polyglandular Syndrome (APS-1 and APS-2) and Immunodysregulation Polyendocrinopathy Enteropathy X-linked (IPEX)
|
|
APS-1 |
APS-2 |
IPEX |
|---|---|---|---|
|
Inheritance Pattern |
AR |
Polygenic |
X-linked |
|
Gene Associated |
AIRE |
HLA allele DR allele |
FOXP3 |
|
Age of Presentation |
Infancy 3-5 years old Early adolescence |
20-40 years old |
|
|
Associated Diseases |
Chronic mucocutaneous candidiasis Hypoparathyroidism Addison's Disease |
Addison's Disease Thyroid disease T1DM
|
Immune dysfunction Polyendocrinopathy Enteropathy Treatment and Screening: Treatment is primarily focused on the underlying diseases. Family members of patients with APS-2s should have thyroid function tests every 5 years due to the most commonly found endocrinopathy being hypothyroidism.
Multiple endocrine neoplasia (MEN1 and MEN2) |
Treatment and Screening: Treatment is primarily focused on the underlying diseases. Family members of patients with APS-2s should have thyroid function tests every 5 years due to the most commonly found endocrinopathy being hypothyroidism.
Multiple endocrine neoplasia (MEN1 and MEN2)
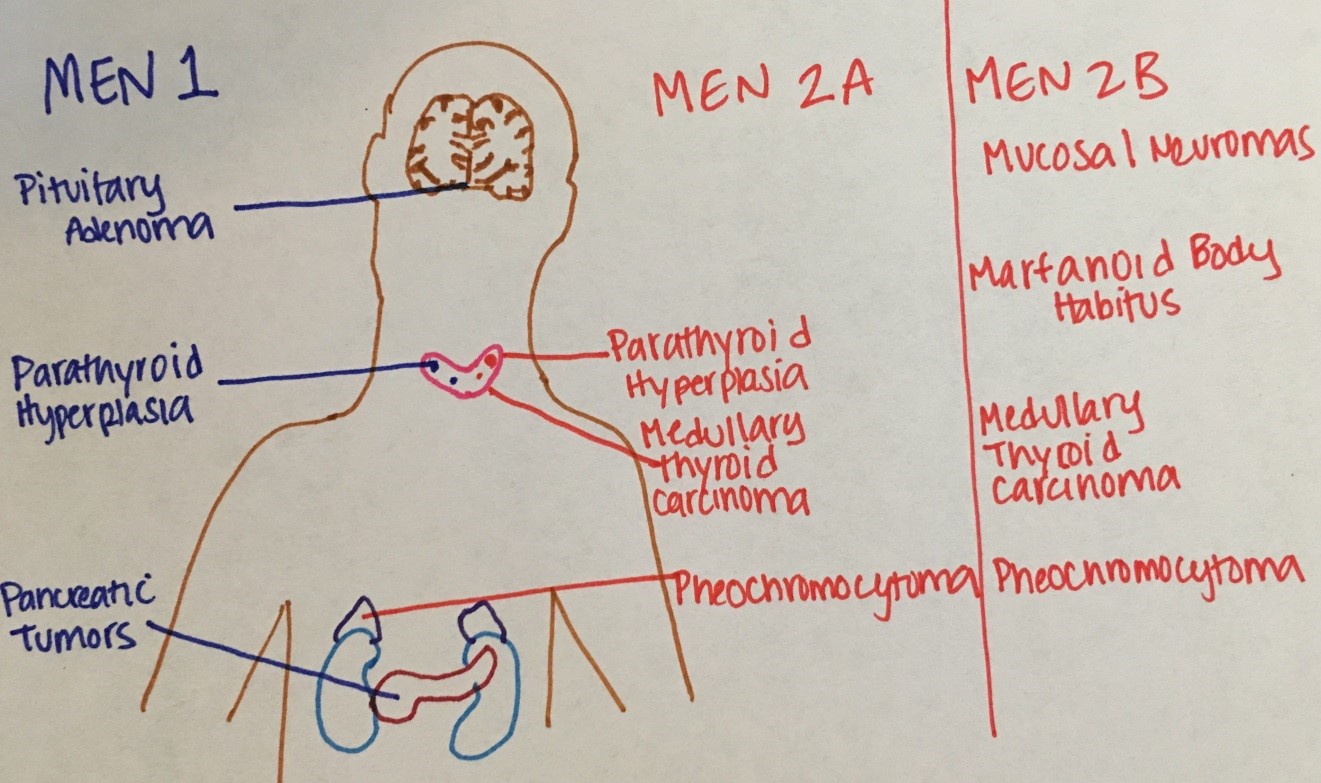
Figure 19. Comparison of MEN type
Etiology: MEN 1 follows an autosomal dominant inheritance pattern due to a mutation of the MENIN tumor suppressor gene. It is rare before the age of 10 years and typically peaks in the second and fourth decades of life. MEN2 also follows an autosomal dominant inheritance but associated with a RET gene mutation.
Symptoms and Diagnosis: Hyperparathyroidism is typically the presenting feature of MEN1. Suspected patients should have screening labs that include serum calcium, prolactin, gastrin, and pancreatic polypeptides. Signs that are consistent with hypercalcemia include lethargy, depression, constipation, kidney stones, and shortened QT interval on ECG. Symptoms of pituitary tumors include findings consistent with prolactinomas (galactorrhea or sexual dysfunction), acromegaly, hyperthyroidism, Cushing's disease, and visual disturbances. With MEN1, you may find high PTH, calcium, gastrin, insulin, and VIP on biochemical studies. MEN2 typically has high calcitonin related to medullary thyroid carcinoma and elevated plasma or urine catecholamines related pheochromocytoma. Imaging of the pancreas and pituitary should also be obtained.
Treatment: Primarily focused on treating the underlying diseases. Family members should be screened, as well, due to the inheritance pattern and high penetrance.
McCune-Albright Syndrome
This syndrome is defined by a clinical triad of fibrous dysplasia of bone, café au lait spots, and precocious puberty. Growth hormone excess, hyperthyroidism, and Cushing Syndrome can also be seen. Associated with mutation of GNAS.
Treatment: Fibrous dysplasia can be followed clinically with annual imaging of the skull and mandible and annual hearing/vision testing. Sometimes, surgery or bisphosphonates may be warranted in severe cases. Precocious puberty is typically treated with aromatase inhibitors or estrogen agonists. Close monitoring is required for testicular lesions in males.

