



Mineral disorders
Calcium, phosphorus, vitamin D, and the hormones that regulate them are very important in skeletal development and mineralization. Abnormalities in these can disrupt calcium homeostasis and therefore cause disorders of mineral metabolism or skeletal disorders of childhood.
Calcium homeostasis
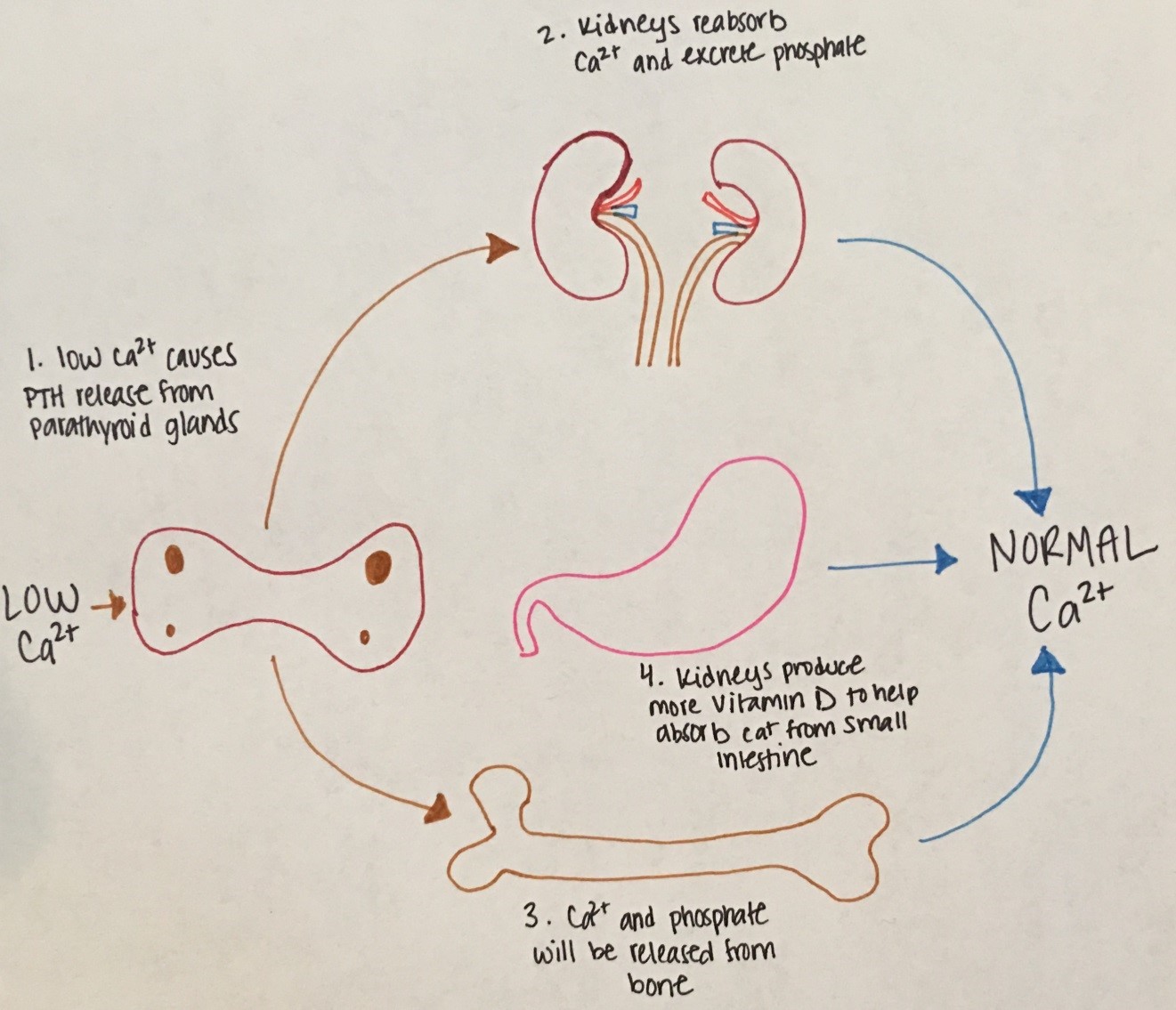
Figure 15. Low serum calcium stimulates release of PTH from the parathyroid glands. PTH stimulates calcium release
from bone and the kidneys to reabsorb calcium. The kidneys also excrete phosphorus and produce more vitamin D.
Vitamin D stimulates intestinal absorption of calcium.
Hypocalcemia
Etiologies:
|
Types |
Physiology |
Examples |
|---|---|---|
|
Neonatal Hypocalcemia |
|
|
|
Illness |
|
|
|
Hypoparathyroidism |
|
|
Table 6. Etiologies of Hypocalcemia
Diagnosis: Measure serum calcium and vitamin-25OHD with corresponding phosphorus and PTH. Also, magnesium and alkaline phosphatase should also be checked. An ECG should be obtained to evaluate for changes related to hypocalcemia (i.e. prolonged QT interval).
Treatment:
- Acute management: IV bolus infusions of calcium gluconate with continuous infusion of elemental calcium
- Chronic management: Oral calcium, calcitriol, and a low phosphorus formula (Similac PM 60/40).
Hypercalcemia
Etiologies:
|
Types |
Physiology |
Examples |
|---|---|---|
|
Familial hypocalciuric hypercalcemia |
Hypercalcemia with elevated PTH, normal phosphorus, normal magnesium, elevated alkaline phosphatase, and low urinary calcium |
Mutation of CaSR gene |
|
Williams Syndrome |
Elevated calcium and calcitriol |
Facial anomalies, cardiac and renal defects, hyperacusis, and cognitive impairment |
|
Hyperparathyroidism |
Elevated calcium, elevated PTH, low phosphorus, and elevated calcitriol |
Childhood neck irradiation |
|
Immobilization |
Decreased skeletal mineral Elevated serum calcium and urinary calcium |
Prolonged immobilization Weightless space travel |
|
Malignancy |
Osteoclastic activity leading to excessive calcium release from bone |
Lymphomas Squamous cell carcinoma Breast cancer Renal cell carcinom, bladder carcinoma Multiple myeloma |
Table 7. Etiologies of Hypercalcemia
Diagnosis: Measure calcium, phosphorus, PTH, magnesium, Vitamin-25OHD, and alkaline phosphatase. ECG will show shortened ST segment and heart block.
Treatment: Increase urinary excretion of sodium with furosemide. Start calcitonin to indirectly inhibit osteoclastic bone resoprtion or inhibit bone resorption directly with bisphosphonates.
Metabolic Bone Disease
Rickets occurs when there is defective mineralization of the epiphyseal growth plate. Although there are different causes of rickets, all forms show characteristic widening and flaring of the epiphyses.
Etiologies:
|
Causes |
Examples |
|---|---|
|
Vitamin D deficiency |
|
|
Calcium Deficiency Rickets |
Unclear underlying causes |
|
Rickets of prematurity |
|
|
Hypophosphatemic Rickets |
|
Table 8. Etiologies of Metabolic Bone Disease.

