



Puberty
Normal female puberty. The hypothalamus-pituitary-ovarian (HPO) axis gradually increases in activity from the prepubertal age causing increases in LH, FSH, estradiol, inhibit A, and Inhibin B. These changes will eventually result in ovarian estrogen production and as a result breast growth, nipple and areola development, female body habitus, cornification of the vaginal epithelium, and enlargement of the uterus.
Normal male puberty. The increasing rise of LH and FSH causes an increase in testosterone, estrone, estradiol, androstenedione, 17-hydroxyprogesterone, Inhibin A, and DHEA. LH and FSH act directly on the testes to stimulated Leydig and Sertoli cell proliferation. Testicular testosterone causes enlargement of the penis, broadening of the shoulders with narrowing of the hips, deepening of the voice, beard growth, temporal hair recession, and thick/curly truncal hair.
Assessment: Tanner staging (or sexual maturation staging) by inspection and palpation is used to assess the sexual maturity of the child.
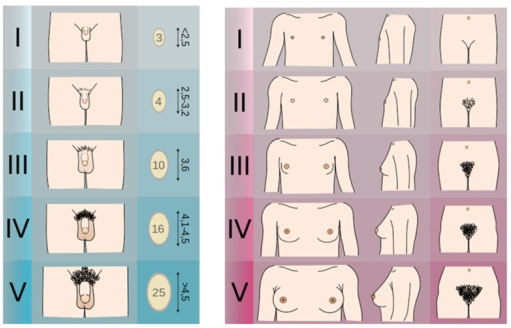
Figure 14. Tanner Stages
from https://openi.nlm.nih.gov/detailedresult.php?img=PMC4478390_fnhum-09-00344-g001&req=4
Definitions:
The onset of puberty in girls is defined by thelarche (breast budding) and it is typically between 8 and 12 years of age, although it can be as early as age 6 years in African American females. Puberty onset in boys is defined by gonadarche (testicular enlargement) and it is typically between 9 to 14 years of age. This is based upon data of predominately Caucasian children, but recent statistics reveal that other ethnicities may have earlier onsets of puberty. *
* Reference: AAP and Pediatric Endocrine Society, Precocious Puberty: A Guide for Families. 2012. https://www.aap.org/en-us/Documents/soen_precocious_puberty.pdf
Adrenarche: increased adrenal androgen production measured by DHEAS. It precedes gonadarche and pubarche.
Gonadarche: increased activity of the HPO axis
Pubarche: onset of sexual hair growth
Thelarche: onset of breast development
Menarche: onset of first menstrual period
Disorders of Puberty
Precocious puberty
Precocious puberty is when the physical changes of puberty (thelarche with other secondary sex characteristics for girls, and gonadarche for boys) begin before the lower age limit for that sex, which is < 8 years for girls and < 9 years for boys. The lower limit is lower for other ethnicities such as African American or Mexican-American. Causes of precocious puberty can be gonadotropin dependent or gonadotropin independent.
Incomplete precocious puberty
Incomplete precocious puberty is isolated premature thelarche in girls < 3 years of age, isolated premature adrenarche, or isolated pubarche with slightly advanced bone age.
Etiologies:
|
GnRH-Dependent or Central |
Examples |
|---|---|
|
Idiopathic |
Sporadic or Familial |
|
CNS Abnormalities |
Acquired, Congenital |
|
Tumors |
|
|
Secondary to chronic exposure to sex steroids |
|
|
Reversible forms |
Space occupying or pressure associated lesions |
|
GnRH-Independent or Peripheral |
|
|
Genetic Disorder |
CAH, Gonadotropin-independent puberty, McCune-Albright |
|
Tumors |
Adrenal sex steroid secreting, Gonadotropin-producing, Ovarian, Testicular |
|
Limited or reversible forms |
Chronic primary hypothyroidism, CAH, Exogenous sex steroid or gonadotropins, Ovarian cysts |
Table 4: Etiologies of Precocious Puberty
Diagnosis: Evaluation includes suggestive physical exam findings, imaging in the form of bone age x-ray (typically advanced for chronological age), MRI of the head, pelvic/testicular ultrasound, and labs including LH, FSH, estradiol, testosterone, DHEAS, Free T4, TSH, and a GnRH stimulation test.
Treatment: includes treating the underlying cause, and if the cause is gonadotropin-dependent, then GnRH agonist therapy may be appropriate.
Delayed puberty
Delayed puberty is defined as lack of testicular enlargement by age 14 in boys and lack of thelarche by 13 in girls, no menarche by age 16, or no pubertal progression for 3 years after the onset of puberty. Delayed puberty can be due to central etiology (hypogonadotropic hypogonadism) or peripheral etiology (hypergonadotropic hypogonadism). Delayed puberty is most commonly due to "functional" hypogonadotropic hypogonadism such as in constitutional delay of growth and puberty, chronic illness, anorexia nervosa, etc. Pathological causes of delayed puberty can be divided into categories of primary hypothalamic-pituitary dysfunction and primary gonadal disorder.
Etiologies:
|
Etiologies of Pubertal Delay |
Examples |
|---|---|
|
Constitutional |
|
|
Hypergonadotropic hypogonadism |
|
|
Hypogonadotropic hypogonadism |
|
Table 5. Etiologies of Pubertal Delay
Diagnosis: Evaluation includes a physical examination, bone age XR, FSH/LH/testosterone/estradiol levels, cranial MRI, pelvic ultrasound, and karyotyping or genetic studies.
Treatment: short course of IM testosterone to trigger ("jump start") puberty in boys, oral estrogen/progesterone for puberty induction in girls. Long-term hormone replacement therapy may be needed in both sexes based on the nature of the problem and possibly continued androgen replacement therapy. Treatment for girls includes cyclic estrogen and progesterone.

