



Diabetes insipidus
The neurohypophysis, or posterior pituitary gland, secretes vasopressin (AVP), also known as anti-diuretic hormone (ADH). AVP is synthesized by the supraoptic and paraventricular nuclei of the hypothalamus (see picture below), in response to plasma osmolality, intravascular blood volume changes (like bleeding, third spacing, etc.) and non-osmotic stimuli (e.g., nausea, drugs).
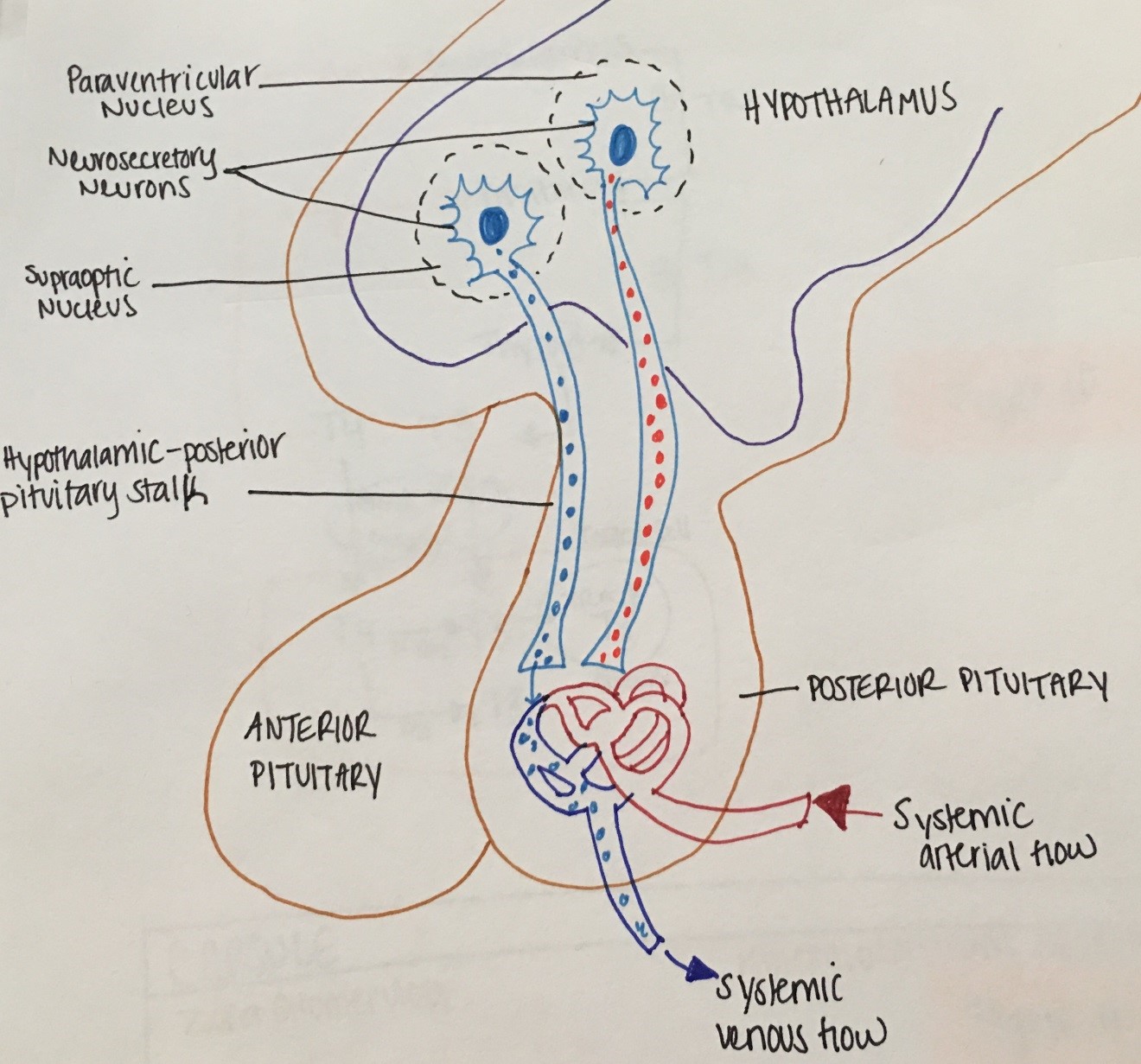
Figure 5. Physiology of the Hypothalamus and Posterior Pituitary
The antidiuretic effect of ADH is regulated through V2, cAMP dependent- receptors and aquaporing-2 proteins inducing increased water permeability and increased urea movement on the collecting ducts. In addition, ADH increases the rate of absorption of sodium (NaCl) in the thick ascending loop of Henle.
Diabetes insipidus (DI) is clinically defined as passing large volumes of hypotonic fluids (> 30ml/kg/24 hours with urine Osm < 300 mOsm/kg and specific gravity <1.010). DI can be central (due to deficiency of functional ADH) or nephrogenic (due to kidney inability to respond to the action of ADH). ADH may also be physiologically suppressed as a result of water overload (primary polydipsia). In contrast, in diabetes mellitus (DM), polyuria is due to osmotic diuresis (urine is hypertonic).
Etiology: Central DI or nephrogenic DI can be complete or partial, familial or acquired (e.g. brain tumor in central DI and lithium in nephrogenic DI).
Symptoms: polyuria and polydipsia, enuresis, FTT/poor growth, unexplained fevers, constipation
Diagnosis: elevated serum Na in patients with abnormal thirst mechanism and dilute urine (as above) vs failure to concentrate urine after a water deprivation test in patients with normal Na/ intact thirst mechanism
Treatment: monitor/maintain fluid balance (drink water as needed) and use ADH-agonists to prevent nocturia and minimize sleep disruption. ADH agonist include L-arginine Vasopressin (natural AVP-subcutaneous), DDAVP (synthetic- intranasal, IV or subcutaneous, or oral) and thiazide diuretics.
Syndrome of inappropriate secretion of ADH (SIADH)
SIADH is due to excessive ADH secretion producing inappropriate urinary concentration and water retention, resulting in euvolemic hyponatremia.
Etiology: CNS disorders (head injury, CNS tumors, hydrocephalus etc.), pulmonary conditions (infections, cystic fibrosis), ectopic production (lung cancer etc.) drugs (thiazides etc.).
Symptoms: headaches, nausea, seizures, focal deficits
Diagnosis: low serum Na, low serum Osm, absence of signs of hypovolemia like tachycardia or hypervolemia like edema and ascites, absence of hypoadrenalism or hypothyroidism (that can also cause euvolemic hyponatremia)
Treatment: fluid restriction and drugs (e.g. vaptans- block ADH binding to V2 receptors)

