



Growth disorders
Physical growth refers to bodily changes that happen as a child matures including weight, length or height and head circumference increases. Growth failure is by far one of the most common reasons for referrals to the pediatric endocrine office.
Linear growth is most rapid in prenatal life when it is mainly regulated by maternal and placental factors. Postnatal growth is progressively slower and predominantly reflective of childs own genetic potential (see growth velocity figure). Another growth acceleration occurs at puberty.
|
What is normal linear growth? |
|
|---|---|
|
0-1 years |
25 cm |
|
1-2 years |
10 cm/yr |
|
3-5 years |
7 cm/yr |
|
4-7 years |
6 cm/yr |
|
7 years - puberty |
5 cm/yr |
Table 1. Linea growth by age
Measurements
Accurate measurement can not be overemphasized in the evaluation of the short child.
Height and Length:
- Patients < 2 years of age are measured lying flat on a board with one fixed and one moving end. The measurement is then plotted on the "birth to 36 month" growth chart. The most accurate growth chart for children under 2 years of age is the World Health Organization growth chart. (https://www.cdc.gov/growthcharts/who_charts.htm#The%20WHO%20Growth%20Charts).
- Patients > 2 years are measured standing up against a calibrated wall stadiometer and plotted on the "2 to 20 year" growth chart.
- Ideally, height or length is measured thrice and the average is calculated.
Growth Velocity: Growth velocity (cm/yr) = (Height2-Height1) / (#months between times) x 12. It determines normal or abnormal growth by comparing height change over a period of time to gender-appropriate norms.
Body Proportions:
- Arm Span (AS) is the distance from one end of child's arm (measured at the fingertips) to the other. AS is measured fingertip to fingertip while standing flat against a wall with arms outstretched. At birth, AS is less than length by about 2.5 cm. By 10 years of age, AS is equal to height; and after 10 years in boys and 12 years in girls, AS exceeds height by up to 5 cm. If AS is greater than 5 cm, pathologic causes of tall stature such as Marfan's Syndrome or hypogonadism should be considered.
- Upper to lower segment ratio (U/L) reflects trunk vs legs ratio, where lower segment is the distance from the middle of pubic symphysis to the floor level and upper segment is height minus lower segment. At birth, U/L is about 1.7:1 or trunk longer than legs. U/L then decreases by 0.1 for every year of age until 10 years of age when it becomes 1:1 (trunk=legs). After 10 years, the ratio is <1.3. U/L segment is high in rickets, Turner, and achondroplasia and low in Marfan Syndrome and eunochoid habitus.
- Weight to length ratio (w/l) or BMI (Body Mass Index) is useful to assess pediatric overweight and obesity. BMI is calculated by dividing the patient's weight in kilograms by their height in meters squared. A BMI between the 85th to 95th percentiles is defined as overweight, and a BMI greater than the 95th percentile defines obesity. It is also informative for the differential diagnosis of short stature (e.g., w/l >1 and with short stature may suggest endocrinopathy, w/l <1 and with short stature may suggest nutritional deficiencies).
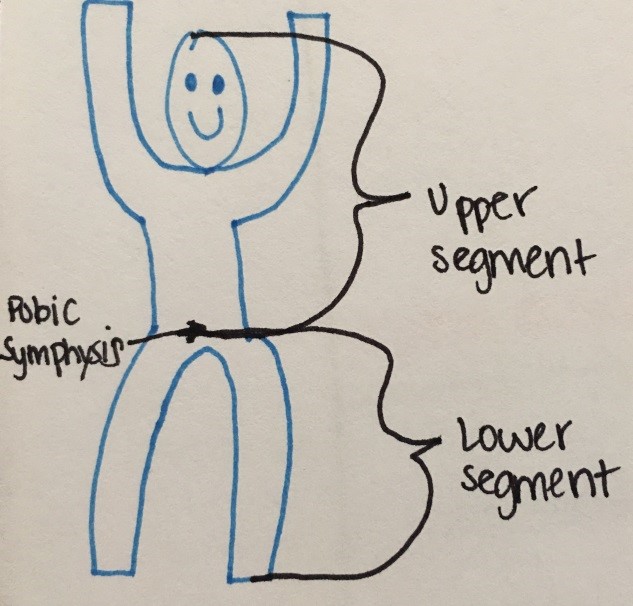
Figure 6. Measuring Upper to Lower segment ratio
Mid-parental height (MPH): measure of child's genetic height potential, using parents adult heights.
Mid parental height calculation:
- Males = [mother's height (in) + father's height (in) + 5 inches]/2
- Females = [mother's height (in) + father's height (in) - 5 inches]/2
- Normal genetic height range is MPH +/- 3.5
Bone Age x-ray: tool for assessment of skeletal maturation as it compares to the chronological age and for the prediction of child's final adult height (for films older than age 6 years). Bone age x-ray is typically delayed in thyroid hormone and growth hormone deficiency or constitutional delay of growth, normal in familial short stature and advanced in precocious puberty.

Figure 7. Example of bone age x-ray.
Children < the 3rd %ile on the growth chart or > 2 standard deviations below MPH deserve a short stature evaluation.
Short stature etiology
Common parental concerns about height tend to be gender biased (e.g. boys that are the shortest in their class or girls that are "too tall" or "taller than even her male classmates"). Referral for a short stature evaluation is also commonly prompted by concerns over bullying/ teasing at school for child's size/stature.
Normal variants
- Familial short stature. Parents are short; therefore, their children are likely to be short. Growth velocity is typically normal along with body proportions, labs and bone age. However, since some pathological causes of short stature are familial, an evaluation may be warranted for children who are very short on the growth chart despite growing along their genetic target height trajectory
- Constitutional growth delay ("late blooming"). Children's growth velocity is usually normal in childhood but progressively declines and it can be associated with delayed puberty. However, catch-up growth occurs without assistance and children eventually achieve heights within their genetic target height range (although typically below their mid-parental height). Bone age x-ray is typically delayed for chronological age.
Pathological causes
- Nutritional deficiency: Undernutrition (global nutritional deprivation or marasmus, inadequate protein intake or Kwashiorkor, anorexia nervosa, zinc deficiency)
- Psychosocial dwarfism: Extreme emotional deprivation can result in failure to thrive (both poor height and weight growth) or even short stature with normal BMI.
- IUGR or small for gestational age: Poor growth due to maternal, placental or chromosomal factors. About 10% of children born SGA fail to "catch-up" to normal growth percentiles by age 2 years.
- Systemic disease: malabsorption, heart disease, renal disease, heme/onc disease, pulmonary disease, diabetes mellitus, inborn errors of metabolism, chronic infection, inflammatory disease
- Chromosomal abnormalities/genetic syndromes: Turner Syndrome, Prader-Willi Syndrome, Russel Sliver Syndrome, Noonan Syndrome
- Skeletal dysplasias: achondroplasia or hypochonodroplasia etc.
- Endocrinopathy: thyroid hormone deficiency, growth hormone deficiency, Cushing Syndrome
- Chronic drug intake: supra physiologic glucocorticoid exposure, high-dose estrogens or androgens, stimulent medications (e.g., methylphenidate, dextroamphetamine)
- Idiopathic short stature: Height < 2 SD below the corresponding mean height for a given age, sex and population group without evidence of systemic, endocrine, nutritional or chromosomal abnormalities
Diagnosis: Bone age x-ray (to assess skeletal maturation), CBC, CMP, ESR, UA to screen for systemic disease, free T4, TSH, IGF-1, and IGFBP-3 to screen for endocrinopathy. Celiac screen optional, Pituitary/brain MRI as needed. Karyotype/microarray or specialized genetic testing as clinically indicated.
Treatment:
Typically, growth hormone replacement is reserved for true growth hormone deficiency. Many causes of short stature are due to an underlying disease and by treating this disease, you are simultaneously able to treat the short stature. For example, levothyroxine treatment for hypothyroidism and growth hormone for growth hormone deficiency typically restores linear growth. However, growth hormone treatment is also FDA approved for Turner Syndrome, small-for-gestational age with failure to catch up, Prader-Willi Syndrome, idiopathic short stature, SHOX gene haploinsufficiency, Noonan Syndrome and chronic kidney disease.
Tall stature is defined as predicted adult stature greater than two standard deviations above the mean height for age and gender. Tall stature can represent a normal variant of growth such as familial tall stature or it may be pathological.
Etiologies:
|
Etiologies |
Example |
|---|---|
|
Genetic |
|
|
Acquired |
|
|
|
|
Syndromic Overgrowth |
|
|
|
Table 2. Common causes of pahological tall stature
Diagnosis: Bone age x-ray, thyroid function tests, fasting insulin level

